
Authors
G. Shikwambane-Ntlemo1,4, S. Jada2 , M. Moncho 1,4, T. Nkonyane3, M. Nchabeleng1,4
Affiliation:
Case Presentation
This is a case of a 49-year-old male patient who presented to the emergency department with one week history of right flank pain. On further enquiry, the pain started in the right iliac fossa, it was initially non migratory in nature and later progressed to involve the whole right side of the abdomen and lower back. He also complained of vomiting, fever and constipation but no obstipation. On examination, the patient was acutely ill with a pyrexia of 38,50C. He had a tachycardia of 125 beats /minute, and a saturation of 93% at room air with normal blood pressures. Physical examination revealed truncal obesity with rebound tenderness and localized guarding of the right hypochondrium , flank and iliac fossa. Examination of the other systems was normal.
Initial investigation showed raised inflammatory markers, a white cell count of 12.90 X 109/L, a C-reactive protein of 356 mg/L and a Procalcitonin of 12,81 ug/L. An urgent abdominal X-ray was ordered, which showed non-specific dilated small bowel loops with air fluid levels and extra visceral gas (Fig 1).
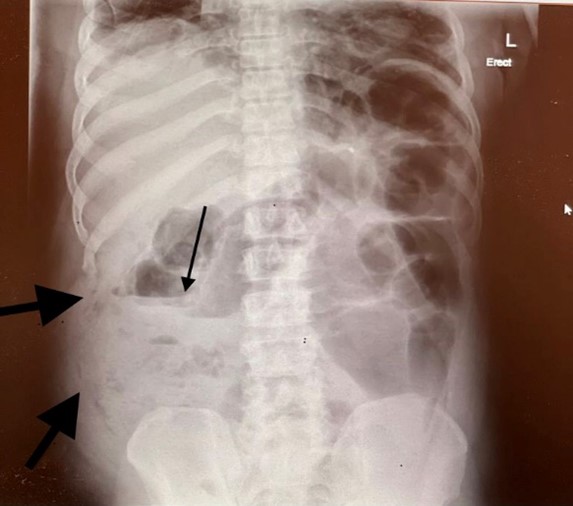
Fig
1: Erect abdominal X-ray showing dilated small bowel loops, air fluid level and
extra visceral gas.
Ultrasound showed an enlarged liver measuring 14cm without the identification of the appendix. Abdominal computed tomography (CT) scan showed a collection in the right iliac fossa with gas and fat stranding on the right iliac fossa (Fig 2). Urine dipstick and and Xpert® SARS-CoV-2 were negative.
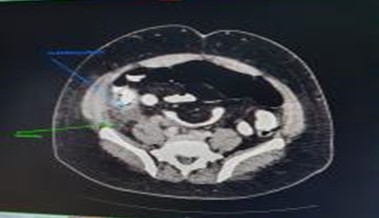
Fig 2. CT scan of the abdomen showing fat stranding (green arrow) and a collection (blue arrow) in the right iliac fossa.
What are the differential diagnosis?
Discussion of the differential diagnosis
1. Complicated acute appendicitis
Acute appendicitis is an inflammation of the vestigial vermiform appendix. It is one of the most common causes of acute abdomen and also one of the most frequent indication for emergency abdominal surgical procedures worldwide(1).
The most common symptom of appendicitis is abdominal pain, which typically begins as periumbilical or epigastric pain migrating to the right lower quadrant (RLQ) of the abdomen. This pain migration is the most discriminating feature of the patient's history (1). Atypical presentation of appendicitis can be as a result of the position of the appendix (1).
Complicated appendicitis is defined as a perforated appendix, periappendicular abscess or peritonitis. Patients usually present with a fever of more than 380C and signs of generalized peritonitis(2). Nausea and vomiting occurs in 50% of the patients (3).
Our patient had a fever of more than 380C with signs of generalized peritonitis on examination hence complicated appendicitis was first on our list of differential diagnosis. However, he had an atypical presentation in that he had right flank pain which was non migratory and progressed to involve the entire abdomen.
2. Complicated colonic malignancy
Colon cancer is one of the most common malignancies. Most guidelines recommend screening at the age of 45 to 50 years of age. It is always considered in patients who present with a change in bowel movements like constipation. Other symptoms include abdominal pain,weight loss and rectal bleeding. A complicated colon cancer may present with signs of bowel obstruction or perforation with generalized peritonitis. Our patient had constipation and signs of generalized peritonitis on examination and CT scan findings of an abscess collection. The differential was excluded by CT scan findings and histology results.
Clinical course and management
The patient was resuscitated and taken to theatre for laparascopic exploration which was subsequently converted to a midline laparotomy on confirmation of a necrotizing infection of the retroperitoneum. Intra-operative findings revealed a ruptured retrocecal appendix. Appendecectomy and debridement of the retropertoneum were perfomed. Pus drained intraoperatively and blood cultures were sent for microbiological investigation. Tissue was sent for histology. The abdomen was left open and the patient was admitted in the intensive care unit (ICU) on ionotropic support. He was started on intravenous amoxicillin-clavulanic acid empirically. A relook laparatomy was planned in 48 hours.
The first relook done on postoperative day two revealed a progressive necrotizing fasciitis and pyomyositis of the right anterior abdominal wall. Extensive debridement of all muscle layers was done from the subcostal rib to anterior superior iliac spine and redebridement of the retroperitoneum was also done. The abdomen was again left open and a second relook was planned in 48 hours ( Fig 3).

Fig 3: Shows open anterior abdomen with a modified bogota bag.
The patient was discharged from ICU to a general ward the following day. At this point the final culture results were released. Blood culture was positive for extended spectrum beta-lactamase (ESBL) producing Escherichia coli (E. coli) and the pus was positive for the same E. coli and an Enterobacter cloacae complex (polymicrobial). The treatment was escalated to meropenem. On post-operative day four in the ward, the patient developed respiratory distress and was taken for a second relook. The infection had extended to the right hemidiaphragm which was debrided, an inter-coastal drain was inserted and the patient was re-admitted to ICU. The repeat tissue samples were still positive for the same organisms.
On post-operative day six, the patient was taken for a third relook, which revealed a perforated caecum, but the necrotizing fasciitis and pyomyositis were resolving. A right hemicolectomy was done with an end ileostomy performed. Repeat tissue samples were sent for microbiological investigation and also for histology and the abdomen was still left open. A multidrug resistant Acinetobacter baumannii complex and group D streptococci were isolated from the tissue cultures. Histology done confirmed that there were signs of peritonitis and pyomyositis and there were no signs of malignancy. The treatment was not modified since the patient was responding well on meropenem.
On post-operative day twenty the patient was discharged from ICU to a general ward in a stable condition. The patient is still in the ward, all inflammatory markers are down, the wound is granulating well (Fig 4).
The plan is to allow full recovery of the patient and a multidisciplinary approach is needed to reverse the stoma and to perform abdominal wall reconstructive surgery.

Fig 4: Anterior abdominal wound showing granulation tissue.
Final diagnosis
The final diagnosis was complicated acute appendicitis with necrotizing fasciitis and pyomyositis of the right anterior abdominal wall, retroperitoneum and hemidiaphragm due to a polymicrobial bacterial infection.
Discussion
Complicated appendicitis such as perforation with abscess formation and localized four quadrant peritonitis occur in about 15% of patients(1). However, the combination of a perforated appendicitis with ensuing necrotizing fasciitis and pyomyositis of the anterior abdominal wall, peritoneum and the extension of the infectious process to the hemidiaphragm is very rare.
Necrotizing fasciitis is a necrotic infection involving deeper layers of the skin and subcutanenous tissue that spread rapidly along the fascia, progressing rapidly to systemic sepsis. It is most commonly induced by injury. The most common microbiological aetiology is polymicrobial although monomicrobial aetiologies associated with very specific pathogens (e.g. Streptococcus pyogenes, Vibrio vulnificus, Staphylococcus aureus) are well-described. Pyomyositis is a pyogenic infection of the skeletal muscles with abscess formation and haematogenous spread.
In conclusion, the diagnosis of complicated appendicitis can be challenging because the presentation is not always typical. Its clinical course can result in a catastrophic outcome if there is a delay in the diagnosis and proper management of complications such as necrotizing fasciitis and pyomyositis. The management requires extensive debridement and administration of appropriate intravenous antibiotics based on culture results.
Early diagnosis and surgical intervention can reduce the morbidity and mortality associated with the condition.
Recommended reading
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®