
Dr Gill Sorour (Paediatric Infectious Diseases) Rahima Moosa Mother and Child Hospital, Johannesburg

Lateral Neck Xray: Showing loss of normal lordosis
Her condition deteriorated in the ward and she became unable to swallow liquids or her own saliva. She was referred for a paediatric opinion.
On examination she was opisthotonic and fully orientated. She was apyrexial and besides a tachycardia, the rest of her vital signs were normal. Examination of her cardiovascular and respiratory systems was normal. Her abdomen was rigid but there was no tenderness. She had a stiff neck and increased tone in her arms and legs but normal reflexes.
CT brain: Normal.
Lumbar puncture: Pressure=9mmHg, no cells, protein=0.17g/L and glucose=3.17mmol/L
Normal calcium, magnesium and phosphate.
During insertion of a nasogastric tube for nutritional support, she became stiff, apnoeic and desaturated. She was treated for a presumed epileptic seizure with phenytoin.

She had two further episodes of stiffening with significant obstruction of breathing. An EEG was normal. The second episode of spasms required CPR and she was intubated.
Differential Diagnosis?
1. Dystonic reaction
Reversible extrapyramidal effects occurring after
administration of a neuroleptic drug or central dopamine antagonist. Characterized
by muscle spasms of the face, neck, and torso. Pronounced fixed eye deviation
and lateral head turning is characteristic. Biperiden can reverse the spasms
but was not available.
2. Strychnine poisoning
Ingestion or inhalation of strychnine poison causes severe seizures in a conscious patient, usually appearing within 5 minutes to 1 hour after ingestion.
3. Severe hypocalcaemia
Physical findings include Chvostek sign (twitching of facial muscles after percussion of facial nerve) or Trousseau sign (carpopedal spasm induced by inflation of a blood pressure cuff).
4. Neuroleptic malignant disorder
Caused by neuroleptic medications or atypical
antipsychotic drugs. Characterized by generalized muscular rigidity and
autonomic instability. Fever may be present. Consciousness is usually impaired.
5. Stiff person syndrome
Rare neurologic disorder characterized by severe muscle rigidity. Generalized spasms can be precipitated by movements, noise, touch, or emotional stimulation. It does not include trismus or facial spasms and responds quickly to diazepam.
6. Tetanus
A nervous system disorder characterized by the gradual onset over 1 to 7 days of hypertonia, trismus and painful severe muscular spasms. As the disease progresses, the painful generalized severe muscle spasms are often aggravated by any external stimulus. There can be associated autonomic dysfunction.
Final Diagnosis
and Management
A diagnosis of tetanus was made once all other causes were excluded, and the child was referred for intensive care management. Her clinic card showed that she had missed her 6-year booster Td vaccination. There was no history of a penetrating skin injury but a healed lesion was noted on her anterior thigh which the mother said was due to a laceration from a barbed wire fence.

Human tetanus immune globulin was not available, and she was given pooled intravenous immunoglobulin as well as a tetanus toxoid vaccine. She received benzodiazepines for muscular spasms and required intubation for 3 weeks and underwent a tracheostomy. She never developed any autonomic instability. She has recovered fully.
Discussion
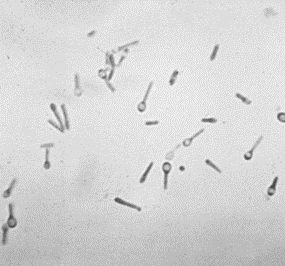
Tetanus is a nervous system disorder characterised by muscle spasms caused by the toxin tetanospasmin that is released by Clostridium tetani, a large spore-forming, obligate anaerobic, gram-positive bacillus. It is present in soil, and in the intestinal tract and feces of various animals.
Mandell
Textbook; Ch 244
C.
tetani enters the body through a break in the skin and anaerobic conditions
allow germination of spores to produce tetanus toxin. The portal of entry is not clear
in up to 23% of patients.
1. Generalised Tetanus
Intense, painful spasms of the masseter muscles and an inability to open the mouth (trismus) is characteristic of tetanus. Nuchal rigidity and dysphagia can occur early and are often associated with risus sardonicus, the scornful smile of tetanus, resulting from facial muscle involvement. As the disease course progresses, patients have intermittent reflex spasms in response to minor stimuli. Tonic contractions cause opisthotonos. During these episodes, patients are fully awake and have severe pain. The upper airway can be obstructed and even the first such spasm may be fatal. Autonomic dysfunction usually occurs after several days and is the leading cause of death. Vasoconstriction, tachycardia and hypertension can alternate with episodes of sudden hypotension, bradycardia and asystole. The severity of illness may be decreased by partial immunity which is probably the case in our patient. Recovery takes another month.
The diagnosis of tetanus is made clinically once all other causes are excluded. Strychnine poisoning is the only condition that really mimics tetanus. Anti-tetanus antibodies are undetectable in most tetanus patients, but there have been reports of tetanus in patients with antibody levels above the commonly cited “protective” concentration of 0.01 IU/L.
2. Neonatal Tetanus
Neonatal tetanus occurs when there is contamination of the umbilical stump due to unclean practices in an infant who does not have protective passive immunity from their mother. Prevention is via immunisation of women with tetanus toxoid during every pregnancy and via employing hygienic practices around umbilical cord care.
Management of Tetanus
The treatment goals of tetanus are to prevent disease progression and to provide supportive and symptomatic care.
1. Disease progression
2. Supportive and Symptomatic Care
Tetanus disease duration varies, averaging 4 to 6 weeks. The overall fatality rate for generalized tetanus is 10% to 20% with optimal care; without access to ICU and mechanical ventilation, mortality rates in adults exceed 40%. Case fatality approaches 100% in the absence of medical intervention
Tetanus is easily prevented by adequate immunization, prophylactic wound management and by hygienic practices during childbirth and neonatal care.
Recommended Reading
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®