
Kubheka S1, Birkett F1, Munian L1, Naidoo KL1, Banoo ZB1, Naidoo V1, Chinniah K1, Archary M1
1Department of Paediatrics and Child Health, University of KwaZulu-Natal
Case Presentation
A four-year-old male presented with a six-day history of fever and rash, followed by five days of loss of appetite, mouth sores and abdominal pain. He had diarrhoea for one day with no vomiting. His viral exanthem was managed at a hospital trauma outpatient unit but, as the fever was not settling, the child was taken to another hospital. The child lives with his paternal grandmother. Both his mother and aunt tested positive for SARS-CoV-2 a month before presentation and self-isolated without contact with the child. The child had not been to day-care since the national lockdown commenced. The child had no symptoms suggesting COVID-19 in the past month.
Examination
He looked ill and was irritable with a fever of 38.5°C although well perfused with regular saturation in room air. His tachycardia BP was normal on admission. He was puffy with oedematous hands and feet (Figure 1) with an erythematous maculopapular rash on the trunk and limbs (Figure 2) and non-tender cervical lymphadenopathy of one centimetre. Conjunctivitis and stomatitis were noted (Figure 3). His abdomen was tender over the right upper quadrant without peritonism and was distended with ascites. His cardiac and respiratory examination was normal with neurology without any meningism.

Figure 1. Pedal oedema

Figure 2. Erythematous maculopapular rash

Figure 3. Stomatitis and fissuring
What is the differential diagnosis?
Differential diagnosis
Management and progress
The patient was initially investigated for sepsis and viral infections. He commenced on Ceftriaxone and Clindamycin to cover for bacterial sepsis. Given the inadequate response to antibiotics and paracetamol and the evolving clinical picture with worsening mucosal involvement, Kawasaki and MIS-C were thought to be the likely diagnosis.
Mention investigations that would support the diagnosis of MIS-C?
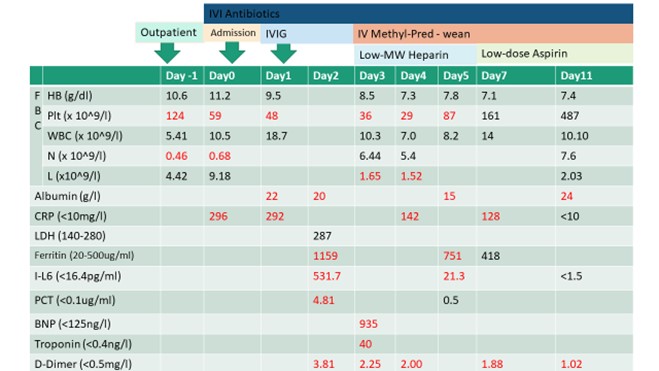
Further workup for hyper inflammation was in keeping with MIS-C. Intravenous immunoglobulin (IVIG) was given at a dose of 1g/kg a day two days after admission and repeated on Day 3. The ECG showed tachycardia without features of myocarditis, and a normal cardiac echocardiogram. His cardiovascular status remained normal. Given the persistent fever, pulsed Methylprednisolone at 10mg/kg was commenced intravenously, which was weaned slowly when the patient started improving clinically. Proton pump inhibitor for gastric protection was commenced, and Heparin at an infusion rate of 10 iu/kg/hr was initiated based on a thromboelastogram and D-dimer in keeping with a hypercoagulable state. Heparin was substituted with low dose aspirin on Day 7. Blood cultures were negative. Urine had protein 2+ and leucocytes 3+ but no growth in the absence of antimicrobials. Viral studies, including measles, were negative. Defervescence was only noted on Day 7 of admission, and the patient was changed to oral prednisone. Inflammatory markers normalised by Day 11 of admission. Antibiotics were stopped by Day 10 though no cultures were positive. The stomatitis and oedema also resolved by Day 11. Abdominal pain and discomfort settled with inflammatory markers though ascites took a week longer to resolve. The patient was subsequently weaned off prednisone over two weeks. Final Diagnosis was MIS-C with a Kawasaki like phenotype. The patient was discharged a week later.
Final Diagnosis
Multi-inflammatory syndrome in children associated with COVID-19
Table 1. Laboratory investigations and management
Additional investigations
Discussion
Since the initial reports of an outbreak of a novel respiratory syndrome in China and identifying the causative organism - SARS-CoV-2 on 31 December 2019, children only accounted for a minority of reported symptomatic infections in most countries. The United States of America and the United Kingdom (UK) reported infection rates of less than 2% in children while in South Africa, the infection rate in children 18 years and below was 6 % before the peak. These differences are primarily due to the testing bias favouring individuals presenting with symptomatic disease. In most countries, children were less likely to have severe illness or die from COVID-19, and in South Africa, earlier reports from the NICD were similar to worldwide reports.
While acute COVID-19 infection in children is mostly asymptomatic or mild, there is an increasing concern of hyperinflammatory complication as reported in the UK and termed Paediatric Inflammatory Multisystem Syndrome – Temporally Associated with SARS-CoV-2 (PIMS-TS). The WHO has subsequently modified the case definition of PIMS-TS, which is now referred to as Multisystem Inflammatory Syndrome in Children and Adolescents (MIS-C) related to COVID-19 (see Table 2). The true incidence is unknown, but MIS-C appears to be a rare complication that may, without appropriate treatment, lead to mortality.
Though the presentation may mimic Kawasaki disease (KD) or Toxic shock syndrome (TSS) and some patients meet these diseases’ criteria, MIS-C is considered a new disease with some differences in pathophysiology. MIS-C is postulated to be as a result of an immune-mediated cytokine storm with myocardial involvement due to direct myocardial injury. While in KD, 80% of cases are below five years, the median age of MIS-C is about 7.3 to 10 years from a meta-analysis of eight studies. Males are more affected than females, with 59% affected in a meta-analysis of studies and up to 78% in a report from Cape Town. Studies reported so far have shown that Black and Afro-Caribbean groups were disproportionately affected by MIS-C in the US, while Hispanic groups were disproportionately affected but proportional to the seroprevalence of COVID-19 in Hispanics. However, the UK reported that Black and Asian groups were disproportionately affected in relation to the number of residents and the number of cases of COVID-19.
The clinical presentation of MIS-C ranges from mild features of hyper inflammation to multisystem involvement with shock requiring respiratory and inotropic support. Most children with MIS-C present with a high fever lasting longer than three days associated with gastrointestinal symptoms, cardiovascular and mucocutaneous involvement after recent exposure to SARS-Cov-2. Other symptoms include non-suppurative conjunctivitis, rash, dizziness, shortness of breath, palpitations and confusion. The presence of gastrointestinal symptoms may mimic an acute abdomen with some patients reported to have a laparotomy for appendicitis. Rashes may vary from morbilliform to erythematous macular rashes with target lesions or pustular rashes, and the distribution of rashes varies. Up to 59% of patients may present with shock requiring inotropic support, and this may not always be accompanied by myocardial dysfunction. Most patients meet the criteria for KD and incomplete KD.
Recent exposure to COVID-19 should be demonstrated, either in history or SARS-CoV-2 antibodies using one of the recently approved antibody tests. SARS-CoV-2 RT-PCR is positive in a small proportion of children presenting with MIS-C (13% - 51%). Antibody testing or serology is likely to suggest exposure with positive results in 75%-100% of all cases. The higher proportion of positive RT-PCRs were likely patients with acute COVID-19 as criteria used were broad, and a high proportion in those studies had respiratory symptoms, which are less common in MIS-C patients. The biochemical markers of MIS-C include thrombocytopenia, lymphopenia in contrast to KD, where thrombocytosis and normal lymphocytes are likely to be present. CRP, ferritin, troponin and D-Dimers are all raised in MIS-C while in KD, the levels are not as high.
Multiple treatment guidelines are available, which are designed with varied available resources. Management in these guidelines is generally similar to that of KD which includes supporting “ABC’s”, IVIG, steroids, aspirin and anticoagulants. Immune modulation therapy may be considered in discussion with a paediatric rheumatologist. One IVIG dose may be sufficient, but a second dose may be required, as about 20% of cases in the Cape Town cohort required the second dose of IVIG. In one study, only 54% of patients received IVIG. Acute kidney injury may also be present, and reports of sterile pyuria have also been documented. Multidisciplinary management including cardiologists, intensivists, infectious disease specialists, rheumatologists and immunologists is advised. High care or ICU care is mandatory in these patients and reported outcomes have been good, with reported mortality ranging from 0-3% of all cases.
This case presentation aims to highlight the clinical condition for front-line clinicians with a high index of suspicion. Early discussion of the case with regional centres with experience in the management of MIS-C and initiating early treatment and meticulous monitoring ensures the best outcomes.
Table 2: WHO MIS-C Case Definition
Children and adolescents 0 – 19 years of age with fever ≥ 3 days
AND 2 of the following:
AND
Elevated markers of inflammation such as ESR, CRP, or procalcitonin.
AND
No other obvious microbial cause of inflammation, including bacterial sepsis, staphylococcal or streptococcal shock syndromes.
AND
Evidence of COVID-19 (RT-PCR, antigen test or serology positive), or likely contact with patients with COVID-19
Additional Reading and references
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®