
L. Richards MBBCh, Mmed(wits), FCP(SA)
J Nel MBChB, FCP(SA), Cert ID(SA), DTM&H
Department of Internal Medicine, division of Infectious Diseases, Helen Joseph Hospital

Figure 1: The patient’s rash on her forehead

Figure 2: The patient’s rash on posterior neck and upper back

Figure 3: The patient’s rash on her chest
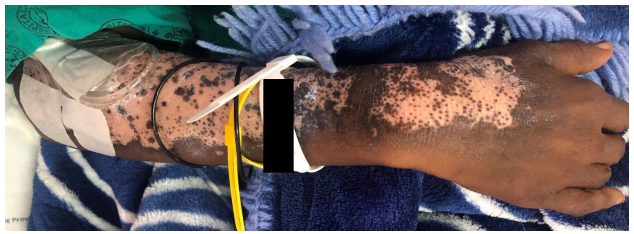
Figure 4: The patient’s rash on her right forearm
She had a CD4 count of 5 cells/µL, an HIV viral load of 287 000 copies/mL and a negative serum cryptococcal antigen. Her sputum GeneXpert MTB/Rif Ultra came back positive for M. tuberculosis, with rifampicin sensitivity
What is the differential diagnosis of this patient’s skin rash?
Photosensitive drug reactions can be ‘phototoxic’ or ‘photoallergic’. Phototoxic reactions look like a severe, well-demarcated sunburn, occurs within minutes to hours of sun exposure and causes a burning sensation. Photoallergic reactions are a type IV hypersensitivity reaction occurring 24-48 hours after sun exposure. It is usually eczematous in appearance and is associated with pruritus. Some of the drugs implicated in this syndrome are sulphonamides, NSAIDs, pyridoxine and efavirenz1. This could be a possibility in our patient as she may previously have been on efavirenz or cotrimoxazole. Factors against this diagnosis are the fact that it did not start out as a well demarcated rash, it is not eczematous, was not pruritic or painful and it has not improved since stopping these medications (if she were ever on them).
Management
The patient was started on rifampicin, isoniazid, pyrazinamide, ethambutol and pyridoxine for her pulmonary tuberculosis. Her lopinavir/ritonavir dose was doubled and a skin biopsy was performed. She was asked to follow up with dermatology in 4 weeks-time.
Final diagnosis
The skin biopsy confirmed a diagnosis of actinic lichenoid leukomelanoderma of HIV.
Discussion
It is estimated that 5% of HIV reactive patients have some form of photosensitive dermatitis. The differential diagnoses include photosensitive drug reactions, CAD, pellagra, lichenoid photoeruptions, porphyria cutanea tarda, pseudoporphyria, photoaggravated granuloma annulare, actinic prurigo and actinic lichenoid leukomelanoderma1.
Recommended reading
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®