
Dr Prenika Jaglal
A case of ventriculo-peritoneal shunt infection due to colistin heteroresistant Acinetobacter baumannii
Case courtesy of Dr Lesego Mothibi, Dr Prenika Jaglal and Dr Jeanette Wadula, Department of Clinical Microbiology and Infectious Diseases, Chris Hani Baragwanath Academic Hospital and University of Witwatersrand, Johannesburg.
Case Presentation:
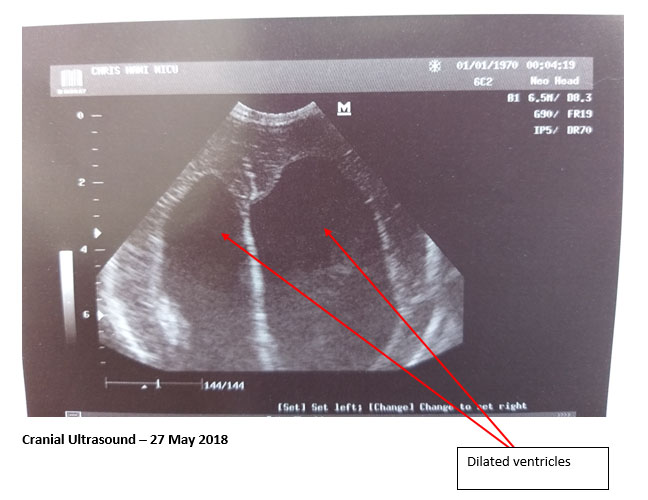
Baby NN was born at Chris Hani Baragwanath Academic Hospital at 37 weeks’ term appropriate gestational age on 26 May2018 by elective Caesarean section. The neonate was found to have a meningomyelocele (MMC) involving the lower lumbosacral region (no cerebrospinal fluid leak) with hydrocephalus and was admitted to the neonatal ICU. Cranial ultrasound showed massively dilated bilateral ventricles (refer to figure below). A CT scan of the brain was booked but not performed due to the patient’s unstable condition. Empiric ampicillin and gentamicin therapy was initiated at birth.
On 30 May 2018, four days post-delivery, a repair of the MMC was performed with insertion of a ventriculo-peritoneal (VP) shunt. CSF specimens were submitted for routine microbiological and biochemical analysis.
Gram-negative bacilli were observed on CSF Gram stain and on 31 May 2018, meropenem was commenced. The following day, an extensively drug resistant (XDR) Acinetobacter baumannii (A. baumannii) was isolated, only susceptible to colistin. A combination of colistin + meropenem was commenced. Patient isolation and strict contact precautions were recommended as infection prevention and control measures. A repeat CSF specimen was submitted for microbiological analysis which yielded the same organism.
A week later, a tracheal aspirate was submitted for MC&S for suspected hospital-acquired pneumonia and a colistin-resistant XDR A. baumannii was isolated. On 12 June 2018, the colistin-resistant A. baumannii was then isolated from CSF.
A few days after the CSF was submitted, the patient underwent wound debridement, washout and VP shunt removal in theatre. On 20 June 2018, an external ventricular drain (EVD) was inserted in theatre. Repeat CSF samples continued to yield XDR A. baumannii resistant to colistin. The CSF and septic marker results appear in the table below.
Investigations: CSF analysis
GNCB: Gram-negative coccobacilli
Colistin susceptibility: ≤ 2 ug/ml, minimal inhibitory concentration (CLSI,M27)
On 30 July 2018, a joint decision between clinical microbiologists and neonatologists to start intrathecal amikacin and colistin was made, taking into account the causative organism’s susceptibility profile, the poor intracranial penetration of colistin, and the reported synergy of antimicrobial agents with successful patient outcomes from anecdotal case reports. The neonate experienced seizures following intrathecal antibiotic therapy; due to concerns of possible neurotoxic side effects, the intrathecal administration of antibiotics was stopped and intravenous colistin and meropenem therapy was continued.
The neonate was extubated and subsequently moved to a step-down ward for palliative care, and a decision made not to resuscitate.
On 5 September 2018, at 68 days of life, the baby demised in the ward after having received 62 days of colistin and 63 days of meropenem.
Clinical microbiological diagnosis: Colistin-heteroresistant Acinetobacter baumannii ventriculitis in a neonate with congenital meningomyelocele and hydrocephalus
Brief discussion about the clinical problem:
Shunt infections are seen in 3% to 20% of patients undergoing ventriculo-peritoneal shunt placement. Ventricular infection from multidrug-resistant (MDR) A. baumannii is a major complication of intracranial procedures with a mortality rate of 71%.
This patient was possibly infected with both colistin susceptible and resistant sub-populations of A. baumannii (heterogeneous population) or developed colistin resistance while on therapy. Heteroresistance was not confirmed according to the current gold standard which is population analysis profiling. Heteroresistance is a term more commonly associated with S. aureus and glycopeptide susceptibility i.e. hGISA/hVISA. It is less well-described in Gram negative bacteria but has emerged as a concern in determination and interpretation of susceptibility results, especially in instances of poor clinical response and where susceptibility results are not categorically conclusive. In A. baumannii heteroresistance to colistin has been attributed to the loss of lipopolysaccharide production. The clinical significance of heteroresistance remains contentious and is difficult to discern given the varied definitions and methodology employed in determination of heteroresistance. However, there is little doubt that subpopulations of bacteria with varied susceptibility to a particular antimicrobial agent play a role in specific infections, especially where there is prolonged antimicrobial use, device-associated infections or chronic infections with source control issues. This is both a diagnostic and clinical challenge in terms of optimizing management.
Intraventricular (IVT) and intravenous (IV) colistin are used as the last resort of treatment of MDR A. baumannii ventriculitis/meningitis due to poor CSF penetration despite inflammation. Colistin-associated neurotoxicity is also a concern, occurring in up to 21.7% of these cases thereby limiting its use. There is no standardised protocol for the management of colistin resistant A. baumannii ventriculitis/meningitis. Whilst case reports offer some guidance, larger studies are needed to define optimal treatment strategies. At present, such cases require an individualised treatment approach.
Question 1 - What are the signs and symptoms of a VP shunt infection?
Answer to Question 2
CSF cell count, glucose, or protein results may not be reliable indicators for the presence of infection in patients with healthcare-associated ventriculitis and meningitis, as these may be normal. A negative CSF Gram stain does not exclude the presence of infection, especially in patients who have received previous antimicrobial therapy. CSF cultures are critical to diagnose healthcare-associated ventriculitis and meningitis.
Question 3 - Can colistin be used intrathecally to treat colistin-resistant A. baumannii ventriculitis?
Answer to Question 3
Several reviews have summarised the use of intrathecal and intraventricular colistin in ventriculitis and meningitis; however, there is no consensus regarding the dosage or length of therapy. Reported dosages of 1.6–20 mg/day given in one or two doses and with duration of therapy ranging from 3 to 56 days have been reported in the literature. Recommendations issued by the Infectious Diseases Society of America (IDSA) for the treatment of bacterial meningitis advise an intraventricular colistimethate sodium (colistin methane-sulfonate) dosage of 10 mg daily for a 21-day duration of therapy for infections caused by aerobic Gram-negative bacilli, although treatment duration should be individualised depending on clinical response.Answer to Question 4
Intravenous colistin crosses into the CSF at a low level of penetration (5% - 25%) despite patients having a disrupted blood-brain barrier. The safe dose of intravenous colistin in neonates and preterm infants is currently not known. According to recent multicentre studies, 2.5 - 5 mg/kg/day and 5.4 ± 0.6 mg/kg/day doses intravenously are considered safe in the paediatric age group and 50,000 - 75,000 IU/kg/day (1 mg colistimethate sodium = 12,500 IU) in newborns and preterm infants. According to the IDSA guideline, intraventricular colistin as a single dose of 10 mg/day has been proposed as safe and efficacious.Answer to Question 5
Tigecycline, a glycylcycline, is not approved for use in the paediatric population. However, it can be a life-saving option as salvage therapy in nosocomial infections due to multidrug-resistant pathogens. Case reports of infants with VPS-related meningitis/ventriculitis report successful outcomes with a tigecycline combination regimen. In one case report, a patient with MDR A. baumannii ventriculitis was treated with a combination of intravenous tigecycline (1.2 mg/kg per dose twice a day) and intrathecal amikacin which was added to intravenous meropenem. Intrathecal amikacin was given for only 7 days and on the sixth day of tigecycline treatment, the CSF was sterilised. There are no available safety and efficacy data from randomised-controlled studies, hence tigecycline must be used in combination as salvage therapy only, for critically ill children where no alternative treatment options exist.References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®