
RN E. Schoeman – Infection Prevention and Control (IPC) Manager at Mediclinic Panorama. Special thanks to RN K. Pienaar (Previous IPC Manager, Mediclinic Paarl) for assisting with some clinical information and to the patient for allowing us to share and learn from her story.
In October 2017, a 26 year old female patient was admitted via the emergency centre at the Health Care facility where she works as a Registered Nurse in the surgical unit. The Health Care Facility is located in the Northern suburbs of Cape Town, South Africa. The patient resides in Paarl, Western Cape. She presented to the emergency department with a fever (39,4˚C), nausea, vomiting, tachycardia, a throbbing headache and diminished sensation of her left arm. She had no other co-morbidities and was not pregnant at the time. She also did not have a recent travel history. On clinical examination no neck stiffness was observed and the chest was clear, however the abdomen was found to be tender. Blood cultures were done, however yielded no growth after 5 days. The urine analysis indicated the presence of blood and protein. Laboratory test included a C-reactive protein (CRP) of 26.9mg/L, Liver Functions Test (LFT) indicated a Gamma-Glutamyl Transferase (GGT) of 76 IU/L and an Alkaline Phosphatase (ALP) of 137 IU/L. On the Full Blood Count (FBC) the Haemoglobin (Hb) was 13,8g/dL, the White Cell Count (WCC) 8.0 x10E9/L and the Platelet count 271 x10E9/L. An ultrasound done of the gallbladder indicated no clear signs of cholecystitis. The patient was treated for flu with an antiviral drug, Oseltamivir (Tamiflu®) and antipyretic medication. She was admitted overnight for observation. The following day the patient was apyrexial and feeling better. The CRP had increased to 98.4mg/L and the WCC decreased to 4.6 x10E9/L. A urine microscopy, culture and sensitivity (MCS) was sent that yielded no growth. The patient was discharged and instructed to return if her symptoms did not improve.
Three days later she was admitted via the emergency centre at another Health Care Facility. The patient presented with a severe headache, tenderness over the abdomen and nausea. Her temperature was 37⁰C and heart rate 136 beats/min. On examination the patient was jaundiced, mildly dehydrated and had diffuse tenderness over the abdomen, especially on the right side. The respiratory system was clear. A urine analysis indicated the presence of ketones, urobilinogen, bilirubin and blood. Laboratory results included a CRP of 196,6mg/L, FBC (Hb - 10.8g/dL, WCC - 7.4 x10E9/L and Platelet count – 10 x10E9/L) and LFTs (ALP – 34 IU/L, Protein – 59 g/L, Globulin – 25 g/L, Total Bilirubin – 186 umol/L, GGT – 368 IU/L, Alanine aminotransferase – 109 IU/L and Aspartate transaminase – 106 IU/L). The patient was admitted to the Intensive Care Unit. A malaria screen was done that tested positive. The patient tested positive for the Plasmodium falciparum and Pan-malaria antigen. After the diagnosis of malaria was confirmed, the patient recalled that she had recently (±16 days prior to becoming ill) sustained a needle stick injury. She had accidently pricked herself with the used stylet after commencing intravenous therapy for a patient that was admitted with Malaria. The index patient tested positive for the Plasmodium falciparum and Pan-malaria antigen with a parasite count of 3.7%. The staff member did not report the needle stick injury at the time of the incident. The patient was treated with Artemether-lumefantrine (Coartem®) over a period of 3 days and discharged after 6 days in hospital.
Malaria
In January 2018 an alert was sent out by the National Institute for Communicable Diseases (NICD) for all physicians working outside malaria endemic area to be attentive for the signs and symptoms of Malaria, as an increase in the number of cases and deaths had been reported (4).
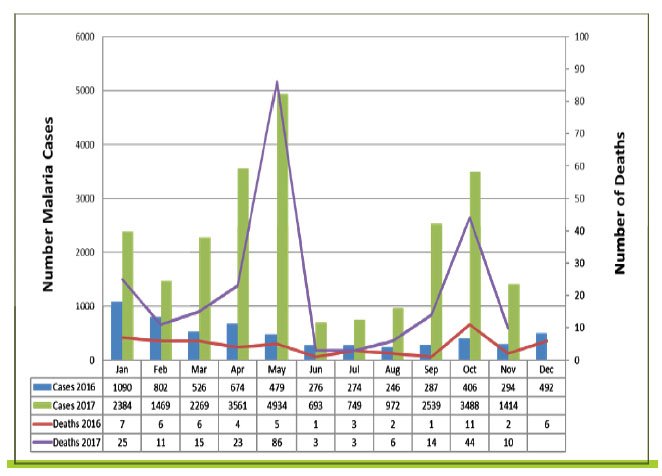
Figure 1: Malaria cases and deaths, South Africa, 2016 and 2017. Source: Communicable Diseases Communique, December 2017, Vol.16(12)
Malaria is a potentially fatal parasitic infection most commonly found in some tropical and sub-tropical countries, and also includes certain areas of South Africa. The incidence of Malaria tends to be higher during the wet, summer months and there are four main parasites that cause this infection (1).
Plasmodium falciparum is the most common malarial infection in Sub-Saharan Africa and is also associated with a more severe form of the disease. There are also four other parasites, that generally cause a milder form of the Malaria, namely Plasmodium malariae, Plasmodium knowlesi, Plasmodium ovale and Plasmodium vivax . The last two parasites mentioned are associated with relapses of the disease if the treatment given is inappropriate (1).
Malaria is transmitted to humans when bitten by an infected female Anopheles mosquito. Once bitten, the mosquito inoculates the malaria sporozoites into the host. The liver cells are invaded by the sporozoites and here they increase and develop further to become schizonts. The mature schizonts ruptures and merozoites are released into the bloodstream and causes breakdown of the Red Blood Cells (RBCs) and is capable of initiating a new cycle of development (1).
Some schizonts (Plasmodium vivax and Plasmodium ovale) can become dormant and remain in the liver for months/years. Relapse of the disease will occur when these dormant schizonts re-activate (1).
Clinical manifestations of malaria present when the RBCs are invaded and ruptured by the merozoites. The infected host will be asymptomatic after the initial mosquito bite and the incubation period can be between 7 and 30 days. The incubation period can by prolonged if the host is taking chemoprophylaxis or some other antibiotics. Once the destruction of RBCs occurs the progress of the disease is quite rapid until effective treatment is initiated or the host demises (1).
Uncomplicated malaria will have mild symptoms, the patient will be ambulant and have normal mental functioning. The patient will not be jaundiced or present with repeated vomiting. The treatment of choice for uncomplicated malaria is artemether-lumefantrine (Coartem®). Primaquine is added to the treatment if Plasmodium ovale or Plasmodium vivax identified (4).
A patient with severe Malaria will present with some of the following clinical manifestations: Jaundice, multiple convulsions, altered level of awareness, hypoglycaemia, respiratory distress, shock, anuria, prostration (lying flat), anaemia, abnormal bleeding. Severe malaria is usually caused by Plasmodium falciparum and the treatment of choice is intravenous artesunate (preferred) or quinine. Once the patient is able to take oral medication Coartem® or doxycycline or clindamycin can be used (4).
For more information on Malaria, please refer to the latest South African Guidelines for the treatment of Malaria, updated 2018.
Outcome of the case:
The patient subsequently had two re-admissions for the treatment of anaemia, pain and fever. She has made a full recovery and was able to return to her normal duties.
A valuable lesson was learned regarding the importance of reporting needlestick injuries, to allow for a thorough investigation to be done after the incident. This will assist in the follow-up of the Health care worker and if post-exposure prophylaxis is required. The Hepatitis B and C Virus and Human Immuno-deficiency Virus (HIV) are the micro-organism most frequently associated with exposure to blood or bodily fluids; however does not include all possible blood-borne pathogens that could result in an Occupational disease (3).
Plasmodium falciparum is a known blood-borne pathogen and inoculation via transfusions and intravenous drug use has been documented. Malarial infections after a needle-stick injury has been reported; however is seldom seen or considered an occupational risk, especially in countries where Malaria is not endemic. This could delay the commencement of effective treatment and have potentially severe consequences for the staff member involved (3).
Refrences
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®