
Unexplained hepatitis in a returning traveller, a case report on Hepatitis E
Table 1
(Abbreviations for Table 1 - TB: Total Bilirubin, CB: Conjugated Bilirubin, ALT: Alanine aminotransferase, AST: Aspartate aminotransferase, ALP: Alkaline phosphatase, GGT: Gamma-glutamyl transpeptidase, LDH: Lactate dehydrogenase, INR: International Normalised Ratio)
Management Antinuclear antibody (ANA) was negative. Patient denied any drug use.
Viral Hepatitis A was excluded with negative IgM. Hepatitis B surface antigen (HepBsAg) and surface antibody (HepBsAb) were negative. However, HepBsAb may in certain cases not be detectable until after a window period of several weeks to months, during which time neither HepBsAg nor HepBsAb can be detected (figure 1)[1]. At this time, the serologic diagnosis can be made by the detection of IgM antibodies against hepatitis B core antigen (anti-HepBc IgM) [1]. Our patient subsequently had a negative anti-HepBc IgM.
Figure 1: Window period of acute HBV infection [1]
(© 2019 UpToDate, Inc. and/or its affiliates. All Rights Reserved)
The National Institute for Communicable Diseases (NICD) was consulted regarded the possible diagnosis of yellow fever. Yellow fever is a vector-borne acute viral haemorrhagic disease caused by an infection with the Yellow Fever virus (YFV). The virus is transmitted by a bite of an infected mosquito vector Aedes aegypti [2]. The laboratory diagnosis of yellow fever is based on the detection of YFV antigen through PCR and serologic assays [3]. The NICD reviewed the patient’s travel history and safely excluded the diagnosis based on no yellow fever risk in the areas she visited. Although yellow fever vaccination is recommended for Kenya, there is specifically no risk in Nairobi (figure 2).
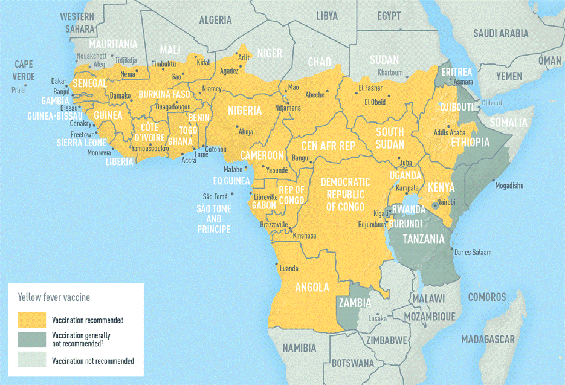
Figure 2: Yellow fever vaccine recommendations in Africa [3]
What is the final diagnosis?
Acute hepatitis E with hepatitis E PCR and IgM positive. Genotyping revealed that the infected virus belongs to the HEV genotype 4 based on phylogenetic analysis. It seems to suggest that the patient acquired the hepatitis E either in South Korea or in the Philippines, and not in Kenya (see figure 3).
Discussion
Hepatitis E was first suspected 30 years ago in Kashmir India where a waterborne outbreak of hepatitis occurred and was found not to be related to Hepatitis A or Hepatitis B virus. At the same time a similar outbreak happened in New Delhi where serology also did not demonstrate either Hepatitis A or Hepatitis B. The confirmation of these observations came in 1983 through demonstration at immune electron microscopy of spherical virus-like particles in stool specimens collected from a human volunteer who had ingested a pooled faecal suspension from patients with acute hepatitis in Afghanistan. [5]
Hepatitis E has a global distribution. It falls in the genus Hepevirus and family Hepeviridae. Based on studies performed on viral genomic sequence, at least 4 genotypes have been described, with one shared serotype. There are two distinct epidemiological patterns. In developing countries such as Asia and Africa with high disease prevalence, it can occur as outbreaks or sporadic cases of acute hepatitis exclusively related to Genotype 1 and 2. The route of transmission is usually faecal-oral in areas with poor sanitation and subsequent water contamination. In developed countries with lower disease prevalence and better water and sanitation supply, sporadic cases of locally acquired Genotype 3 and 4 have been reported. The route of transmission is often zoonotic transmission to humans from consumption of undercooked meat, specifically pork. [5]
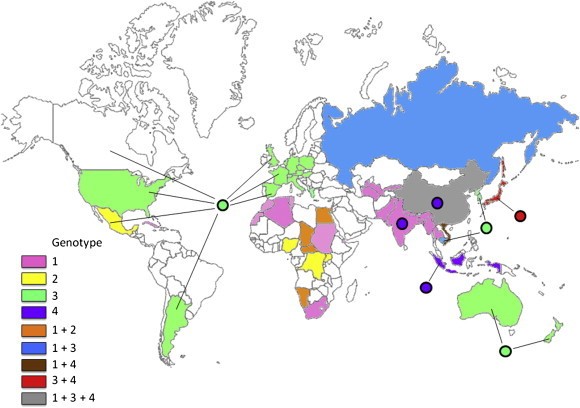
Figure 3: Distribution of HEV genotypes in viral isolates obtained from humans and animals (mainly pigs). The colors used for a country and the circle associated with it represent the predominant HEV genotypes of human and animal isolates, respectively, from that country. The figure is based on data from Okamoto, 2007 [5]
The World Health Organization (WHO) estimate that 20 million HEV infections occur annually, with over 3 million symptomatic cases and in excess of 55 000 HEV‐related deaths, accounting for 3.3% of the total mortality due to viral hepatitis [6]. According to the Centers for Disease Control and Prevention (CDC) mortality in the third trimester of pregnancy reaches 10%–30% [7]. They have found that equally high mortality rate occurs in solid organ transplant recipients on immunosuppressive therapy and in patients with pre-existing chronic liver disease [7].Recommended Reading
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®