
Dr D Steyn, Dr S Potgieter, Dr E Glover
Universitas Academic Hospital
Case Presentation:
A 56yr old female from Bloemfontein was referred to the Department of ENT at Universitas Academic Hospital in November 2018 with a 6 month history of dysphagia, odynophagia, dysphonia and otalgia. Upon presentation she was completely unable to swallow solids and semi-solids.
She had been started on empirical TB treatment in February of the same year after seeking medical attention at a local hospital for marked weight loss and generalized lymphadenopathy. Sputum at that stage was TB geneXpert negative but biopsy of a supraclavicular lymph node showed granulomatous inflammation with caseous necrosis and a histological diagnosis of TB was thought compatible. Unfortunately no tissue samples were sent to the TB laboratory for microbiological confirmation. Despite 9 months of TB treatment she had progressive weight loss, dropping 4 dress sizes. She had no known chronic diseases and was on no chronic medication. She had no significant surgical history and had never smoked or used alcohol. She was born in a rural village in the Eastern Cape and had spent her most of her life there. Her family had moved her to Bloemfontein in the previous year when she had become too unwell to stay alone. She had no travel history and no occupational exposure
Upon examination she was noted to be cachectic with conjunctival pallor. The previously reported generalized lymphadenopathy was not present. She had hoarseness of voice and stridor. She was not able to swallow even saliva due to a large mass at the base of her tongue. Apart from the stridor, cardiopulmonary exam was normal as was abdominal examination.
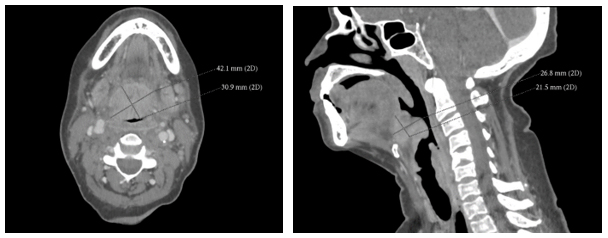
Upon laryngoscopy she was found to have a large mass lesion extending from the right tongue base to involve the epiglottis, posterior pharyngeal wall and larynx. A CT scan of her head and neck was requested and is shown below.
Answer to Question 1
Rhinoscleroma is a rare chronic, slowly progressive infectious disease caused by the inhalation of the gram-negative bacterium Klebsiella rhinscleromatis The organism is endemic in the tropical to temperate zones of Africa, Asia, Eastern Europe and South and Central America, especially in poorer socio-economic settings. Many authors favor the term Scleroma over Rhinoscleroma as although the disease process usually involves the nasal cavity (95% of patients) it can also involve the nasopharynx (up to 43%) oropharynx (13 -35%), larynx (15-40%) and trachea (12%) and bronchi (2-7%). It usually occurs at the transitional regions between two types of epithelium (squamous, ciliary, and respiratory). Risk factors such as crowded conditions, poor nutrition and poor hygiene appear to play an important role in the pathophysiology of the disease but in all other regards patients are immunocompetent.
Answer to Question 2
Answer to Question 3
Answer to Question 4
Infectious granulomatous diseases may include tuberculosis, actinomycosis, syphilis, leprosy, histoplasmosis, sporotrichosis, zygomycosis, blastomycosis, paracoccidoidomycosis and mucocutaneous leishmaniasis. Noninfectious granulomatous diseases include sarcoidosis and granulomatosis with polyangiitis (Wegener granulomatosis). Lethal midline granuloma and other neoplastic conditions need also be considered.
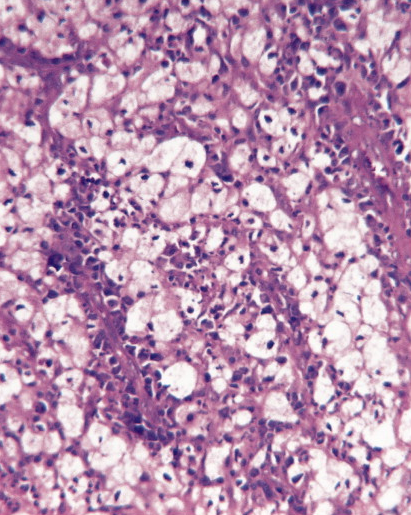
Figure 1: High power H&E stain showing Mikulicz cells – large macrophages with abundant vacuolated foamy cytoplasm
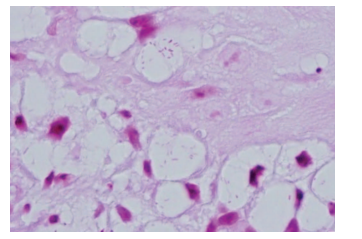
Figure 2: Gram stain: Mikulicz cell containing gram negative bacilli
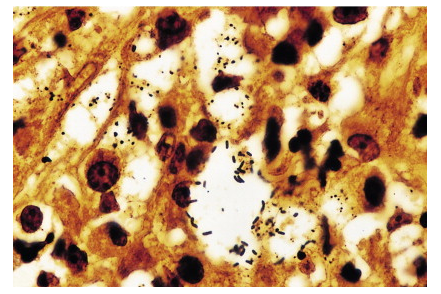
Figure 3: Warthin-Starry Stain showing Klebsiella rhinosleromatis bacilli within the Mikulicz cell
Question 5: How is Scleroma treated?
Answer to Question 5
Rhinoscleroma can be managed effectively with a combination of antibiotics and surgical debridement and repair. Numerous antibacterial agents have been described in the management of Rhinoscleroma, usually used in combination. These include streptomycin, tetracyclines, rifampicin, trimethoprim-sulfamethoxazole, and ciprofloxacin. Relapse rate is high and depending on the stage prolonged treatment is necessary (3 -12 months depending on response)
Continue to outcome of case
References:
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®