
Dr Evan Shoul, Prof Lucille Blumberg, Prof John Frean
Case presentation
A 52 year old man was flown to a Johannesburg hospital from Zambia on 10 January 2018. He had been on holiday in the South Luangwa National Park, having arrived there 2 weeks prior to his transfer to South Africa.
Presenting history:
6 January 2018:
He developed frontal headaches and reduced appetite in the evening.
7 January
By the next morning, his headaches had worsened. He now complained of fever, rigors and backache. He had lost his appetite but had no nausea, vomiting or diarrhoea.
8 January
He developed diarrhoea which was watery with no blood. His right foot became swollen and purple. A local doctor assessed this as cellulitis and prescribed flucloxacillin. A rapid malaria test was negative according to the patient.
9 January
He now noted jaundice with dark urine. The doctor was again consulted, tested his urine and noted ‘bilirubin in the urine’. The patient had generalised myalgia, worsening headaches and further episodes of diarrhoea. A repeat rapid malaria test was negative.
10 January
His headaches continued to worsen along with persistent fever. Myalgias worsened, especially involving his lower back. He also noted bilateral knee pain. He was then transferred via medical evacuation to South Africa.
Systemic enquiry:
Central nervous system – headaches, no neck-stiffness, paraesthesiae over right knee and photophobia noted on day of transfer
Eyes – vision normal, no conjunctivitis noted.
Ear, nose, throat – recent sore throat one week before. No cervical nodes noted. No other ENT issues.
Chest – no cough, mild shortness of breath on moderate exertion. No chest pain.
Abdomen – no nausea/vomiting. No abdominal pain/cramps. Diarrhoea as noted. Appetite reduced since onset of symptoms.
Genito-urinary – no dysuria/no haematuria. Dark urine for 3–4 days despite adequate oral fluid intake.
Musculo-skeletal - bilateral knee and right foot pain 3 days prior to presentation.
Skin - macular rash noted over abdomen over preceding few days.
Background history:
Allergies: nil
Surgical history: nil
Medical history: hypercholesterolaemia – on atorvastatin 20mg daily x 25 years
Also, on sertraline 100mg daily.
No diabetes mellitus/hypertension/epilepsy/asthma.
Social: lives with his wife and 4 children in Melbourne, Australia. Works as managing director of a safety equipment company. Smokes <5 cigarettes a day and drinks at least 4 units of alcohol per day.
Travel history: current trip – family holiday in Zambia, visiting national parks. Staying in upmarket lodges, drinking bottled water, eating prepared food. Reports being bitten by many mosquitoes, flies, “other bugs”. He also travels annually to rural China for business.
Clinical examination:
On admission, awake and alert but acutely ill, uncomfortable and agitated.
Vital signs: heart rate – 120 beats/min, BP 100/60mmHg, Temp 39.5°C, oxygen saturation 94% on nasal prong oxygen at 2L/min. Weight 100kg.
On general examination, he was markedly jaundiced. No nodes, oedema, pallor, cyanosis or clubbing. He was not clinically dehydrated. He had a fine macular rash over his abdomen. He also had numerous small raised erythematous reactions likely secondary to insect bites – mostly over his back, trunk, legs. Chest exam: no distress, resonant, clear
Cardiac exam: pulse regular, good volume. Normal cardiac auscultation.
Abdomen: no distension, soft, non-tender. No organomegaly.
Neuro: GCS 15/15, no focal deficit.

Figure 1: Lesions from bites noted on lower limbs.
Preliminary investigations:
Admission: 10 January 2018
White cell count 3.28 x 109 cells/L
Haemoglobin 12.9 g/dL
Platelets 78 x 109/L
Malaria thick and thin smear – negative
Malaria common antigen – negative
Malaria falciparum antigen – negative
Sodium 132 mmol/L
Potassium 3.0 mmol/L
Urea 7.6 mmol/L
Creatinine 201 µmol/L
Bilirubin (total) 138 µmol/L
Bilirubin (conjugated) 97 µmol/L
Alkaline phosphatase 355 U/L
Gamma GT 436 U/L
ALT 270 U/L
AST 457 U/L
C-reactive protein 376 mg/dL
International normalised ratio 1.3
Question 1: What is the differential diagnosis of fever and thrombocytopenia in a returning traveller?
| Viral: | EBV, CMV, HIV |
| Bacterial: | Ehrlichiosis; anaplasmosis; Babesiosis; miliary TB, brucellosis, relapsing fever, leptospirosis, rickettsial infections, Salmonella spp. |
| Parasitic: | malaria, visceral leishmaniasis, trypanosomiasis |
| Fungal: | histoplasmosis |
| Malignant: | haematological – lymphoma/leukemia, multiple myeloma - myeloproliferative disorders |
| Miscellaneous: | drugs, cirrhosis |
| Rheumatic/inflammatory: | Haemophagocytic lymphohistiocytosis, Gaucher disease |
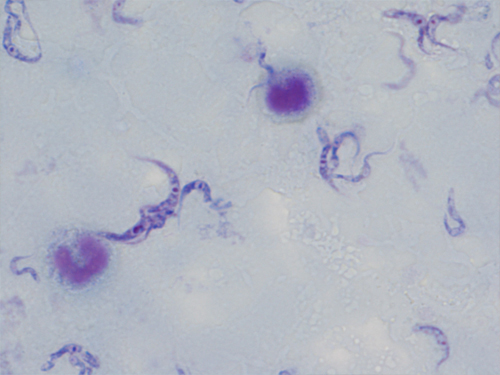
Figure 2: Thick smear of peripheral blood
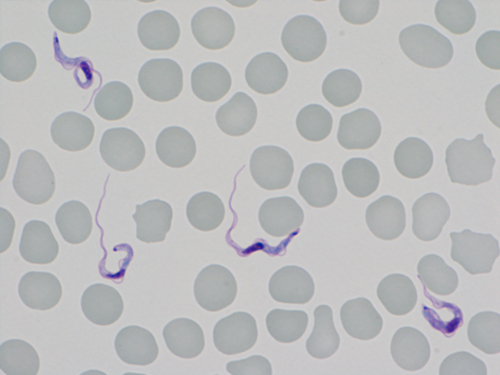
Figure 3: Thin smear of peripheral blood
Question 2: What is the diagnosis?
Answer to Q2
A: East African trypanosomiasis
There are 2 forms of trypanosomiasis: a slow, progressive form endemic to western and central Africa caused by Trypanosoma brucei gambiense (West African trypanosomiasis, WAT) and a more rapidly progressive form caused by Trypanosoma brucei rhodesiense found in eastern and southern Africa (East African trypanosomiasis, EAT).
This patient’s clinical picture, particularly the characteristic chancre, his geographical exposure, together with the findings on peripheral smear, are consistent with East African trypanosomiasis.
Question 3: How is this infection transmitted?
Question 4: What are the clinical features and the different clinical stages of trypanosomiasis?
Question 5: How is the infection diagnosed?
Question 6: How is trypanosomiasis treated?
First stage treatment
Pentamidine: this is the first line option for WAT and maintains more than 95% efficacy despite decades of use. It may be administered intra-muscularly for 7 days or as an intravenous infusion. Adverse effects include hypotension, nephrotoxicity and electrolyte disturbances.
Suramin: this agent is used for first-stage EAT. It is given as a slow infusion in a complex regimen spaced over a month. A test dose is required due to the risk of hypersensitivity reactions. Side effects occur frequently and are mostly reversible. Most often, these include nephrotoxicity, peripheral neuropathy and thrombocytopenia.
Second stage treatment
Nifurtimox-eflornithine combination therapy (NECT) is indicated for second-stage WAT. It has higher cure rates (>95%), lower rate of mortality (<1%) and easier administration with fewer side effects than melarsoprol and eflornithine monotherapy. Gastrointestinal side effects with NECT are very common. Neuropsychiatric effects, such as sleep disturbances, irritability and mood changes along with myelosuppression may also be noted.
Melarsoprol is the only therapeutic option for second-stage EAT but may be used as a salvage regimen for WAT. It has significant toxicity, the most important being an encephalopathic syndrome occurring in around 10% of cases and is associated with a high mortality rate. Co-administration of steroids may prevent or alleviate the encephalopathy. Headache, fever and gastrointestinal complications may also be encountered.
Out come of the Case
Patients require regular follow-up for up to 24 months. This includes clinical assessment and laboratory testing of peripheral smears and CSF as parasites may remain viable for prolonged periods and lead to relapses.
References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®