
Penelope Rose1,2, Ronalda de Lacy1, Elizabeth Goddard1
1 Paediatric Gastroenterology, Department of Paediatrics and Child Health, Red Cross War Memorial Children’s Hospital, University of Cape Town
2 Tygerberg Children’s Hospital, Department of Paediatrics and Child Health, Stellenbosch University
Case history
A one year old girl known with biliary atresia and a well-functioning Kasai portoenterostomy (bile ducts removed and a loop of intestine brought up to replace them) presented with fever and worsening jaundice of a day’s duration. She had been diagnosed with biliary atresia and had a Kasai portoenterostomy performed at the age of 8 weeks. She was also HIV-exposed and on the PMTCT program, but was confirmed PCR negative on three separate occasions. On examination she was found to be pyrexial and jaundiced with firm hepatosplenomegaly but no ascites or peritonism. She was haemodynamically stable, alert and had no evidence of bleeding.
Question 1 - What is the most likely diagnosis and why? What would the appropriate initial investigations and further management be?
Question 2 Which organisms would you suspect? What antibiotics should be used?
She must be commenced on intravenous broad-spectrum antibiotics that will cover Gram-negative enteric bacteria and Enterococcus. In this case we chose a combination of cefotaxime and ampicillin. Ceftriaxone should be avoided as it has may cause biliary sludge and raised liver enzymes.(5)
After 48 hours she had deteriorated, remaining pyrexial and developing respiratory distress requiring nasal CPAP. Her septic markers remained elevated but blood cultures had not grown any organism.
Question 3. If the patient does not improve, what further investigation is indicated?
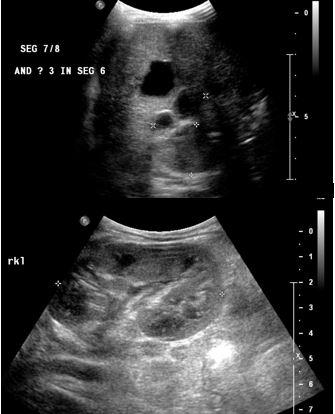
An abdominal ultrasound found multiple intrahepatic biliary collections measuring between 20 x 30mm to 34 x 30mm in size. On previous ultrasounds the liver and spleen had been enlarged, but there were no intrahepatic cysts or bile lakes noted.
The four largest cholangeal abscesses were drained percutaneously under ultrasound guidance. All blood cultures and cultures of pus aspirated from the abscesses were negative. The child’s clinical condition improved post-drainage of the abscesses, her fever resolved and she no longer required any respiratory support. In consultation with surgical colleagues it was agreed to complete a prolonged course of intravenous antibiotics. The duration of treatment for acute cholangitis is at least fourteen days, but a longer duration of three to four months may be needed with liver abscess or recurrent cholangitis, in particular in children with biliary atresia who have a portoenterostomy.(3) Her liver enzymes returned to baseline levels prior to discharge. She was discharged after a three week course of intravenous antibiotics on oral ciprofloxacin prophylaxis.
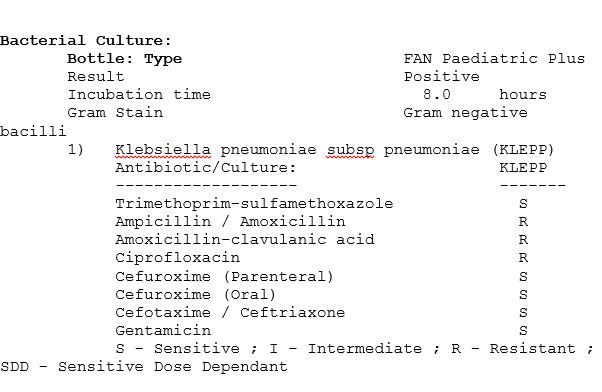
She was followed up as an outpatient and was well until she returned unwell four months later with fever and deepening jaundice. She was readmitted with a presumed diagnosis of cholangitis, reinvestigated and started empirically on intravenous ampicillin and cefotaxime. Blood cultures grew Klebsiella pneumoniae:
Question 4. Why did she re-present with cholangitis?
| Hepatitis A Antibody | Negative |
| Hepatitis B s Antibody | Titre >1000 |
| Varicella zoster virus IgG | Equivocal |
| Measles IgG | Positive |
| Mumps IgG | Negative |
| Rubella IgG | Negative |
Lessons from this case
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®