Answer to Q5
Bobo and Newton first described Capnocytophaga canimorsus in 1976. It is a Gram-negative bacillus found in normal oral flora in dogs and cats. Capnocytophaga canimorsus was previously known as DF-2 (Dysgonic fermenter-2) before being renamed by the Centre for Disease Control in 1989. The term ‘dysgonic’ was used to describe its slow growth in bacterial culture. In fact, the anti-coagulant Polyanethole-sulfonate used in culture medium has been implicated in inhibiting its growth.
C. canimorsus are capnophilic facultative anaerobic, fastidious Gram-negative rods. They are fusiform or filamentous gliding bacteria and are closely related to Fusobacterium and Bacteroides species. C. canimorsus requires large amounts of exogenous iron for growth. It grows slowly on blood (5% sheep blood in Columbia agar) or chocolate agar in 10% CO2. Media has to be incubated at 37.8C for at least 5 days. Colonies may not visible for 2–7 days on blood agar. Recently, the growth medium was optimized (Heart Infusion agar Difco with 5% sheep blood) and the bacteria were shown to grow in 2 days at 37.8C in 5% CO2.
C. canimorsus infection is associated with the absence of a pro-inflammatory response with low cytokine levels and is due to the fact that C. canimorsus does not interact with human Toll-like receptor 4 (TLR4) and is able to down regulate TLR4 and the pro-inflammatory signaling cascade. Not only is C. canimorsus resistant against phagocytosis and killing, it also blocks the killing of unrelated bacteria by macrophages.
Infection is most often transmitted through bites or contact with open wounds, but transmission has been described through contact with intact skin. Infection occurs after an incubation period of 1-7 days. Asplenic patients are at risk of more severe disease and alcohol abuse is another reported risk factor. No obvious risk factor can be identified in 40% of cases. Most infections occur in individuals older than 50 years.
The spectrum of C. canimorsus infections includes gangrene, sepsis, meningitis and endocarditis. Severe sepsis caused by C. canimorsus is extremely rare and mortality can range from 25–30% to as high as 60% in patients with septic shock. 60% of those who develop septic shock die within 30 days. A retrospective single centre Helsinki ICU cohort with a median age of 55.5 years found that 94% of patients with Capnocytophaga canimorsus were coagulapathic and 69% developed Acute Kidney Injury. Unexpectedly, patients with meningitis did relatively well.
Clinical manifestations:
After an incubation period of 1–7 days, patients may experience an abrupt onset of malaise, abdominal pain that might mimic an acute abdomen, confusion, shortness of breath, and rapid progression to severe septic shock. On physical examination patients present with a petechial rash on the trunk, lower extremities, and mucous membranes. The original bite wound classically lacks inflammation. The rash might evolve from purpuric lesions to gangrene. The clinical manifestations of sepsis are secondary to a profound inflammatory response leading to endothelial dysfunction resulting in disseminated intravascular coagulation, acute respiratory distress and organ damage. Cases of fatal acute haemorrhagic adrenal insufficiency (Waterhouse–Friderichsen syndrome), gangrene and purpura fulminans may occur. Individuals aged more than 50 years are at greatest risk. Endocarditis and meningitis are difficult to differentiate from more classical causes other than from the underlying risk factors and exposure history.
Management:
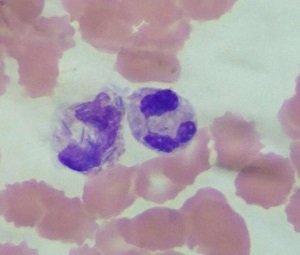
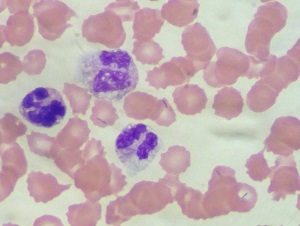
Diagnosis is usually based on clinical history because the bacteria are extremely difficult to grow. Up to 14 days of incubation might be necessary to detect growth on typical media. Peripheral blood smear and observation of abundant intracytoplasmic fusiform rods within neutrophils allows a presumptive diagnosis in the correct setting. Capnocytophaga species infection responds well to penicillin and β-lactam–β-lactamase inhibitor combinations. Other active agents include clindamycin, linezolid, tetracycline and carbapenems. Co-trimoxazole and aminoglycosides are not effective. Because of the relatively aggressive nature of infection and the difficulty in obtaining a laboratory diagnosis, therapy should be started as early as possible.
The patient subsequently developed hospital acquired pneumonia and antibiotics were escalated to Imipenem. The organism is sensitive to Carbapenems. He had a good clinical response and was eventually successfully extubated. He remained dialysis dependent for several weeks after which he was discharged with persistent renal dysfunction, but was not dialysis dependent.