
Dr SE Kubheka, M Archary and R Bobat, Department of Paediatrics Infectious Diseases, King Edward Hospital, University of KwaZulu-Natal
A 12-month-old boy was seen at a urban district hospital in KwaZulu-Natal with a 2-day history of fever, diarrhoea, irritability and abdominal distension. The stools were not blood-stained.
Three days prior to this admission his carer observed a single episode of a generalized tonic-clonic seizure associated with a fever. The infant was taken to the traditional healer where scarification of the body was performed. According to the family the infant improved over the next 2 days.
The rest of the history was unremarkable and age-appropriate vaccinations where up to date. Water source is piped water from a home tap.
On examination, his temperature was 38.5°C, pulse rate 140 beats per minute. He was well perfused but pale and irritable, no jaundice was noted.
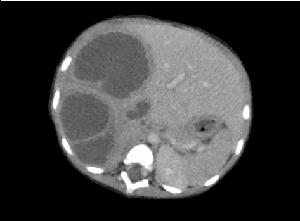
The only clinical abnormality of note was abdominal distention with a 5cm hepatomegaly without splenomegaly. Notably the neurological assessment was normal.
Initial investigations:
Question 1: What do you suspect and what would the next investigation be?
In cases of bacterial liver abscess polymicrobial infection is common.
Empiric therapy should consider specific risk factors and potential causative conditions that may indicate unique pathogens such as norcardia which can occur in patients with chronic granulomatous disease.
Community acquired cases of pyogenic liver abscess can be managed with a third generation cephalosporin. If E. histolytica is considered, metronidazole must be added, in addition to surgical interventions including percutaneous drainage.
Question 3: Which test would you order if a diagnosis of E. histolytica liver abscess is considered?
Question 4: What is the likely diagnosis?
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®