
Answer to Question 1
In sexually active young women, or in cases of sexual abuse, the differential diagnosis includes (most common in bold):Case continued
In the case presented, the treatment did not improve the clinical picture and a second, most likely, seeded lesion developed.
Image 1 (Published with permission of patient)
Red arrow: beefy red ulcer
Yellow arrow: early satellite lesion
Question 2: What is the most likely diagnosis when taking the clinical appearance into consideration?
Answer to Question 2
Donovanosis (granuloma inguinale), classic lesion of a beefy red ulcerAnswer to Question 3
Answer to Question 4
Donovanosis is a predominantly tropical cause of genital ulcer occurring chiefly in small endemic foci in all continents except Europe. Diagnosis requires the careful collection, staining and examination of smears or biopsies of characteristic genital, and occasionally, extragenital lesions for demonstration of the pathognomonic Donovan bodies within histiocytes. The causative organism is Klebsiella granulomatis (formerly Calymmatobacterium granulomatis), which is a Gram-negative, non-motile, pleomorphic bacterium that stains well with Giemsa, Wright, and silver stains. Donovan bodies are dark-staining (bipolar-staining) rod-shaped inclusion bodies seen in the cytoplasm of mononuclear phagocytes or histiocytes. Culture isolation of K granulomatis is difficult and impractical.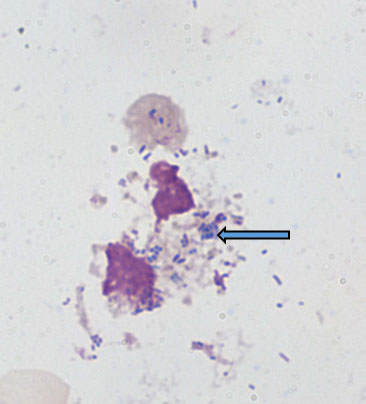
Image 2 with thanks from Prof AW Sturm’s laboratory, Durban, South Africa
(blue arrow pointing at a clump of Donovan bodies (Klebsiella granulomatis))
Reference
Richens, J. 1991. The diagnosis and treatment of donovanosis (granuloma inguinale). Genitourin Med 67(6):441-452
Question 5: How would you treat this patient?
Answer to Question 5
Several antimicrobial regimens have been effective, but only a limited number of controlled trials have been published (O'Farrell. 2002). Treatment has been shown to halt progression of lesions, and healing typically proceeds inward from the ulcer margins; prolonged therapy is usually required to permit granulation and re-epithelialization of the ulcers. Relapse can occur 6–18 months after apparently effective therapy. The Centers for Disease Control and Prevention (CDC) STD treatment guidelines should be followed.
Outcome of the case:
A 6 week course of azithromycin 500 mg orally on alternate days led to complete resolution of both lesions. Her ARVs were changed to second line therapy consisting of AZT/3TC and LPV/r. At 6 weeks: CD4 13 cells/µL, VL < 150 copies.FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®