
FIDSSA case of the month- November 2016
Dr Max Peter Winkler, Hout Bay Family Medical Centre, Cape Town (SASTM)
Acute drug induced hepatoxicity in a patient recently returned from Fiji.
In July 2015 a 20-year old woman presented to general practice with a 3 week history of worsening nausea, loss of appetite and jaundice. She had recently returned from 3 month trip to Fiji where she had been working as volunteer teacher on one of the rural outer islands of the Fijian archipelago. Prior to travel she was seen at a local travel clinic and was immunised for hepatitis A and typhoid fever.
She gave no history of any recent febrile illness but was bitten by mosquitoes while away. She was currently taking a combined oral contraceptive pill that she had started before leaving South Africa, and she was not on any other medication. She admitted to occasional alcohol use and smoking while away. She denied any illicit drug use but does admit to frequently drinking a traditionally prepared Kava drink with the local inhabitants in Fiji “on more days than not”.
On examination the patient was stable and apyrexial, she was jaundiced with some abdominal tenderness in the RUQ and 1-2 cm hepatomegaly. She had a normal CNS examination, and no other signs of acute liver failure were noted.
Table 1 liver Biochemistry results 15/07/15
Autoimmune markers and viral serology for hepatitis A, B and C were all negative. An ultrasound of the liver was normal and no signs of biliary tract obstruction or intra hepatic masses were found.
Q1: What further investigations are neede to make a definitive diagnosis?

Fig 1: Liver biopsy specimen, showing eosinophilic infiltrates and apoptotic hepatocytes.
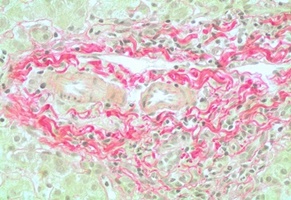
Fig 2: Liver biopsy specimen, a Sirius red stain showing fibrotic changes in the tissues surrounding the portal tracts, also evidence of bile plugging in the canaliculi of the liver.
Q2: What is the most likely cause of the drug induced hepatoxicity in this case?
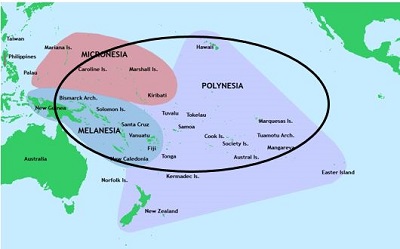
Fig 3 approximate geographic distribution of Kava cultivation in the south pacific
Q4: What is the likely mechanism of hepatoxicity and what are the possible risk factors?
Acknowledgements
Dr G Skead and Prof H Wainwright, UCT division of anatomical pathology for access to and copies of the Histology Slides
Prof W Spearman, GSH department of hepatology for the clinical notes and the management of the patient in the liver unit.
References
Hepatitis induced by Kava (Piper methysticum rhizoma).Stickel F1, Baumüller HM, Seitz K, Vasilakis D, Seitz G, Seitz HK, Schuppan D. J Toxicol Clin Toxicol. 2003;41(2):109-13.
Acute hepatitis induced by kava kava.Humberston CL1, Akhtar J, Krenzelok EP.
Planta Med. 2015 Dec;81(18):1647-53. doi: 10.1055/s-0035-1558295. Epub 2015 Dec 22.
Contaminant hepatotoxins as culprits for kava hepatotoxicity--fact or fiction? Teschke R, Sarris J, Lebot V, MMWR Morb Mortal Wkly Rep. 2002 Nov 29;51(47):1065-7.
Hepatic toxicity possibly associated with kava-containing products--United States, Germany, and Switzerland, 1999-2002. Centers for Disease Control and Prevention (CDC).
Hepatotoxicity Induced by “the 3Ks”: Kava, Kratom and Khat
Flaminia Pantano,Roberta Tittarelli,Giulio Mannocchi,Simona Zaami,Serafino Ricci,Raffaele Giorgetti,Daniela Terranova, Francesco P. Busardò,and Enrico Marinelli, Rolf Teschke, Academic Editor,Phytother Res. 2013 Mar;27(3):472-4. doi: 10.1002/ptr.4729. Epub 2012 May 14, Liver Int. 2010 Oct;30(9):1270-9. doi: 10.1111/j.1478-3231.2010.02308.x.
Kava hepatotoxicity: pathogenetic aspects and prospective considerations.
Teschke R1. Liver Int. 2010 Oct;30(9):1270-9. doi: 10.1111/j.1478-3231.2010.02308.x.
Toxic Hepatitis After Consumption of Traditional Kava Preparation
Stefan U . Christl , MD , Axel Seifert , MD , and Dirk Seeler , MD
Department of Gastroenterology, Asklepios Klinik Harburg, Hamburg, Germany
J Travel Med. 2009 Jan-Feb;16(1):55-6. doi: 10.1111/j.1708-8305.2008.00259.x. http://www.news24.com/SouthAfrica/News/Kava-products-get-MCC-chop-20030822
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®