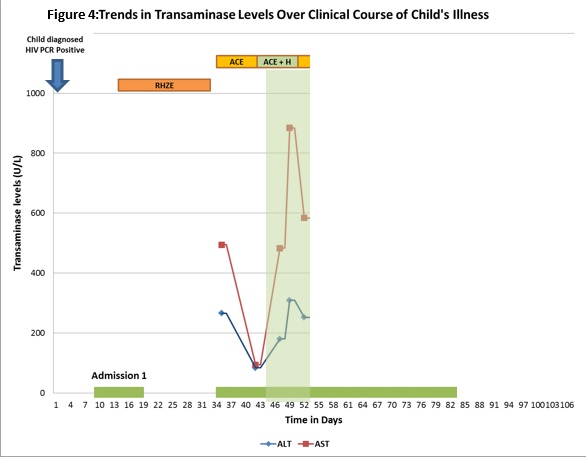
Answer 7: Yes: transaminase levels above five times the upper limit of normal warrant withdrawal of potentially hepatotoxic drugs [2, 4]. In children with clinical evidence of hepatitis (e.g. jaundice, vomiting, right upper quadrant pain), transaminase levels above three times the upper limit of normal warrant withdrawal of potentially hepatotoxic medications.
Differential diagnosis:
- TB drug related liver injury;
- Co-trimoxazole hepatotoxicity;
- Viral hepatitis, including hepatitis A, B, C, cytomegalovirus (CMV), HIV;
- Hepatitis secondary to bacterial sepsis;
- Hepatitis caused by tuberculosis;
- Hepatitis caused by congenital infections, e.g. syphilis.
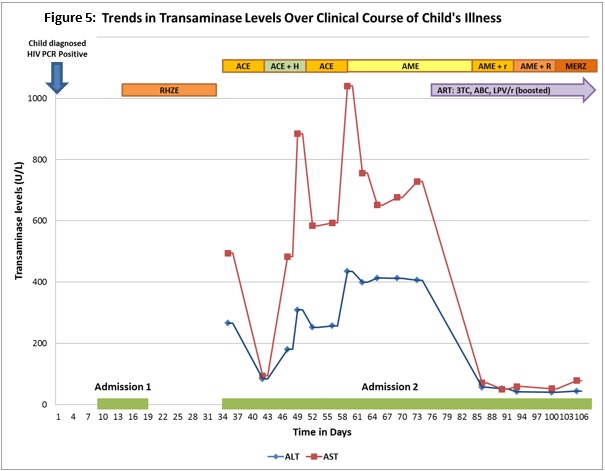
Case continuedIt was decided to discontinue her anti-tuberculosis treatment, in view of the transaminase elevations. ‘Liver friendly’ anti-TB treatment (amikacin, ciprofloxacin – subsequently changed to moxifloxacin – and ethambutol) was continued.
Results of the child’s baseline TB work-up were as follows:
- Gastric aspirate GeneXpert negative for Mycobacterium tuberculosis DNA;
- Two gastric aspirates smear negative for acid-alcohol fast bacilli (AFB) and culture negative for M. tuberculosis.
A work-up for viral hepatitis we conducted, and serology for hepatitis A, B and C were negative. Human cytomegalovirus (CMV) viral load was lower than the detectable limit. Syphilis serology was negative.
ALT and AST were repeated after seven days of discontinuation of the first-line TB regimen: the ALT level was 84 U/L, and ALT was 94 U/L (2.8× and 1.2× the upper limit of normal, respectively). The child’s clinical condition had improved considerably and, as at admission, there were no clinical features of hepatitis.
Question 8: What management option would you adopt at this stage in the child’s clinical course?