
Sean Wasserman - IDSSA
In January 2014, a 35 year woman presented to ophthalmology complaining of ‘a worm’ in her eye. Her examination at that time was completely normal, but she had brought photographs taken with her cellular phone of what appeared to be a subconjuctival worm-like foreign body. She was prescribed a single dose of ivermectin (which she never received) and told to follow up after 9 months.
Question 1: what are the infectious causes of ocular worm-like foreign bodies?
Answer to Q1
IntraocularThe patient returned to ophthalmology in November 2014, again with the problem of a worm in her left eye, but on this visit also described experiencing transient skin swellings. She reported having similar symptoms for the past 5 years and had regularly self-medicated with single doses of albendazole, with no improvement.
The patient lived in Cape Town, worked as a hairdresser and was in a relationship with a male partner. She had no chronic medical problems but was receiving treatment for infertility. She was a migrant from a rural village outside Douala, Cameroon, and had not left Cape Town since September 2011. She had also travelled to Nigeria in 2009 and 2010 for stays under 30 days. She remembered being aware of many flies and mosquitos in her hometown. Her diet consisted of cooked meat and vegetables, always bought from stores, and she never ate raw fish. There were no close exposures to animals.
On examination there was a subconjunctival worm-like structure in the left eye. It was making writhing movements. A 5 cm live worm was removed under local anaesthetic and sent for histology [Fig. 1]. The patient was discharged on a 5 day course of albendazole.

She was called to return to the Infectious Diseases clinic after the department was informed of the pathological findings, and was seen there in December 2014. Her ocular symptoms had resolved but she was having frequent recurrences of intermittent swellings over her right deltoid and right eyelid. Physical examination revealed a discreet soft non-tender raised lesion over her eyelid. A photo she had taken of her deltoid area with her phone showed an erythematous serpiginous lesion [Fig. 2], which had since disappeared.

Figure 2. Serpiginous lesion of migrating adult
Question 2: what is the most likely diagnosis and what is the term for the observed skin lesions?
Answer to Q2
The combination of a crawling eye worm and skin lesions in an immigrant from Cameroon is typical for loiasis, caused by Loa loa. The transient swellings associated with this condition are known as Calabar swellings (episodic angioedema), but adult worms migrating through subcutaneous tissue can occasionally be seen.
Other possible infections in a patient from West Africa presenting with similar skin lesions include:
Question 3: What is the epidemiology and biology of the agent of loaisis?
Answer to Q3
Loa loa is a filarial nematode found in the rainforests of central and West Africa. The endemic countries include: Angola, Cameroon, Central African Republic, Chad, Democratic Republic of the Congo, Equatorial Guinea, Gabon, Nigeria, Republic of Congo, and Sudan.
It is estimated that at around 30 million people live in high- and intermediate-risk areas (with a disease prevalence of 40 and 30%, respectively), and that at least 10 million people are infected with L loa.
The epidemiology of loiasis is influenced by the widespread use of ivermectin for onchocerciasis control, and the highest burden of the parasite is now in areas where O. volvulus is not found. Because of poor vector efficiency, prolonged exposures of months to years are usually required for infection, but loiasis is well-described in travellers to endemic areas.
Loa loa undergoes developmental stages both in humans and the Chrysops fly (also known as the tabanid fly) [Fig. 3], which serves as the intermediate hosts and disease vector.
Chrysops live and breed in the rainforest canopy and lay their eggs in water. They are attracted to smoke from burning wood fires, bringing them into contact with humans.
Third stage L. loa larvae are transmitted by entering a bite wound (which is painful) as the female fly laps up blood from a human host. These microfilariae migrate to subcutaneous tissue where they mature into adult worms after 3 months. Characteristic Calabar swellings result from a local angioedematous response to the migration of maturing larvae and/or adult parasites. The cycle is completed after a pre-patent period of 6 to 12 months when adults produce sheathed microfilariae which are released into the bloodstream and are ingested by flies during a blood meal from the infected human host.
Clinical pre-patency has a wide range, with symptoms appearing from as early as 2 months after infection to 15 years. Microfilariae have diurnal periodicity and circulate in peripheral blood during the day to match the feeding habits of the Chrysops fly. Clinical disease is caused by adult worms as they migrate to any area of the body; this characteristically involves the eye, but mature worms have also been seen in the penis, nipples, or the bridge of the nose, and occasionally in the kidneys and heart. Adults can live for at least 17 years, but are unable to replicate within the human host.
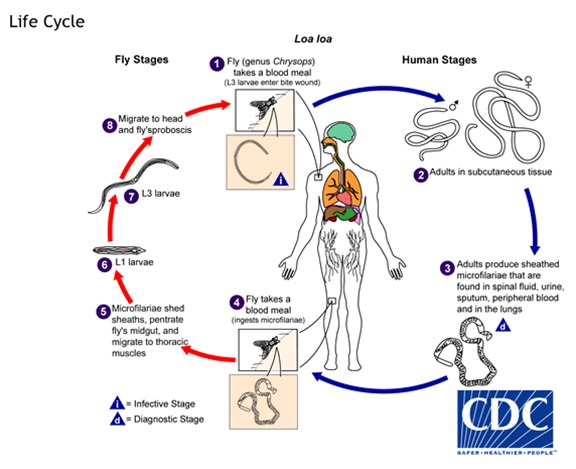

Fig 3. Life cycle of Loa loa and its vector, the Chrysops fly
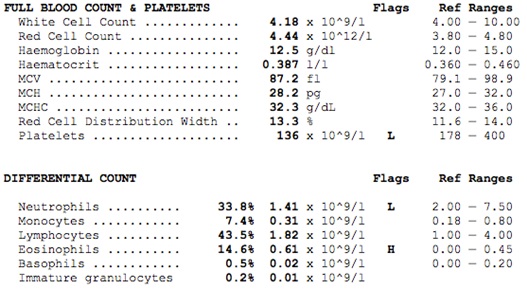
Blood tests were performed which revealed the following:
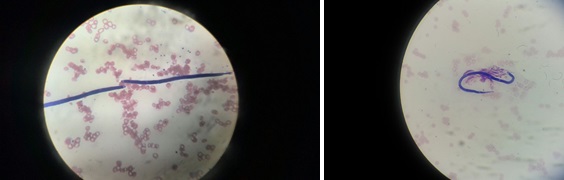
Peripheral blood smear showing typical microfilariae
Question 4: How is L. loa diagnosed?
Answer to Q4
The clinical findings of an adult worm moving across the eye together with Calabar swellings are pathognomonic for loiasis. High eosinophil counts and elevated IgE levels are non-specific but characteristic laboratory findings. Infection with L. loa is confirmed by the detection of microfilariae on peripheral blood smear, which may be thick or thin and stained with Giemsa or hematoxylin-and-eosin (H&E). Microfilariae are 250 - 300 μm long and 6 - 8 μm in diameter; they are sheathed and contain a string of nuclei that extend to the tip of a hooked tail (unlike the microfilariae of Mansonella perstans and Onchocerca volvulus which are unsheathed).
The highest densities of microfilariae are found during daytime hours between 10h00 and 16h00, but over half of patients harboring adults worms have undetectable microfilariae in the bloodstream at any time, making diagnosis difficult in endemic areas. Highly sensitive and specific PCR tests are available, but these may also fail to identify so-called occult carriers. Serological tests are useful for the diagnosis of loiasis amongst travellers and expatriates, but not for those in endemic areas as they remain positive for prolonged periods following infection.
Question 5: Describe the management of loiasis?
Answer to Q5
The management of loiasis involves surgical removal of adult eye worms plus antihelminthic therapy to eradicate the infection and prevent recurrences. Treatment should be offered to all expatriates and travellers, especially if they are symptomatic.
Diethylcarbamazine (DEC), a piperazine derivative, is recommended by WHO as first-line treatment of loiasis. It has an uncertain mechanism of action, but is thought to enhance host immune destruction of microfilariae by either altering their surface membranes or inhibiting release of immunomodulatory eicosanoids. DEC also has macrofilaricidal activity, killing around 50% of adult worms via hyperpolarisation and immobilization; this further reduces the microfilarial burden.
Although it is considered to be the treatment of choice for loiasis, the efficacy and safety of DEC for this infection in patients from endemic areas has not been studied in clinical trials and a single course of treatment results in long term cure rates of only ~ 50% of expatriate visitors to endemic countries. Therefore long term follow-up is required, with retreatment if symptoms recur.
Adverse effects are common and include fever, nausea, arthralgias and flaring of Calabar swellings. This is most likely attributable to a host immune response to the rapid killing of microfilariae and can be reduced by the concomitant administration of antihistamines and corticosteroids. Life threatening reactions such as encephalopathy and shock are uncommon, but may occur in patients with high level microfilaraemia (> 30,000 - 50,000 microfilariae/mL), and are not prevented by anti-inflammatories. Strategies to reduce microfilarial levels prior to DEC therapy include pretreatment with albendazole (or apheresis in exeptional circumstances).
Recommended dosing of DEC for loiasis
DEC is not available in South Africa, and alternative agents are therefore required for the treatment of imported cases of loiasis. Both albendazole and ivermectin have activity against L. loa. Because the parasite does not harbour Wolbachia endosymbionts, doxycycline has no role in the treatment of loiasis.
Similarly to DEC, ivermectin administration results in a rapid immune-mediated reduction of microfilarial load, but is not active against adult worms. Thus it is not curative and carries a risk of severe adverse events, but has been recommended for use in patients with moderate microfilarial densities (2000 - 8000 microfilariae/mL) prior to definitive therapy with DEC.
Albendazole has no significant microfilaricidal activity but prolonged courses have a direct embryotoxic (and possible macrofilaricidal) effect on adult worms, resulting in a more gradual decline of microfilarial levels over a period of months (with no risk of severe adverse events). A 21 day course of albendazole 200 mg twice a day has been effective in patients refractory to treatment with DEC. On the basis of this, and the fact the both DEC and ivermectin are unavailable for human use in South Africa, albendazole is the preferred (and only) treatment option in our setting. Response to therapy should be monitored with blood smears for microfilaraemia, peripheral eosinophil count and clinical symptoms.
The patient was prescribed a 3-week course of albendazole. On review in January 2015 she had no further symptoms and her physical examination was normal. Her peripheral eosinophil count had increased, however to 1.46 x 109 cells/L, but there were no microfilaria seen on peripheral blood smear. She had also tested HIV-seropositive but was in denial about this diagnosis and, despite counselling, was unfortunately lost to follow up.
Reference
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®