
Dr Evan Shoul
(With special thanks to Dr Peter Swart, Consultant Anatomical Pathologist, NHLS Division of Histopathology, Charlotte Maxeke Johannesburg Academic Hospital)
A 55-year-old man was referred from the Dermatology clinic with a diffuse rash. Towards the end of 2013, he noticed subcutaneous lumps over his left upper arm and back, which gradually ruptured through the skin to form scaly ulcers. Some of the lesions were occasionally associated with a purulent discharge. Over the next few months, more lesions developed, now involving his face and legs. Of note, a lesion appeared on his nose, starting as a pimple., which gradually extended into the nasal cavity, eroding through cartilage. It was associated with a thick, purulent and, at times, bloody nasal discharge.
He had attended his local clinic a number of times but had showed no response to courses of oral antibiotics. He had no other significant symptoms. He reported no constitutional symptoms and a systemic enquiry was unremarkable.
He was diagnosed HIV positive in March 2013 at another hospital after presenting with oropharyngeal candidiasis. His CD4 count then was 54 cells/mm3, but he failed to return to the clinic to commence anti-retroviral therapy. He had been otherwise well up until the current presentation and reported no previous episodes of tuberculosis or prior hospital admissions. He was currently on no chronic medication.
He lives alone in Cape Town but travels widely throughout the country for his work. He reports no international travel. His animal exposure includes goats, chickens and stray dogs around his house in a peri-urban settlement. His business requires extensive travel throughout the Western and Northern Cape, including on-site training in forested areas. His colleagues are all well and his family history is unremarkable.
On examination, he was afebrile with mobile, non-tender, soft, generalized lymphadenopathy. His oral cavity was normal but had discrete lesions on the face, trunk and limbs as shown in the following images:


Question 1: What is the differential diagnosis of these skin lesions?
Answer to Q1
Bacteria:
Cutaneous bacterial infections
Mycobacterium tuberculosis, non-tuberculous mycobacteria (M.marinum, M.fortuitum), Mycobacterium leprae
Cutaneous nocardiosis
Fungal:
Mycetoma, chromoblastomycosis, blastomycosis, cryptococcosis
Parasitic:
Cutaneous leishmaniasis
Non-infectious:
Sarcoidosis
Psoriasis
Neoplasms: squamous carcinoma, basal cell carcinoma, mycosis fungoides
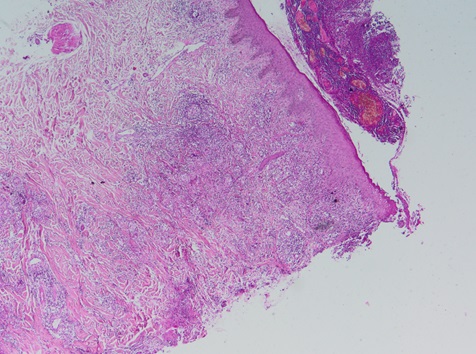
Figure 1. Scanning microscopy of an H&E section (x4 magnification) shows skin consisting of epidermis and dermis with an overlying fibrino-purulent crust. Interstitial dermal inflammation is noted, as well as occasional poorly formed granulomata with multinucleate giant cells.
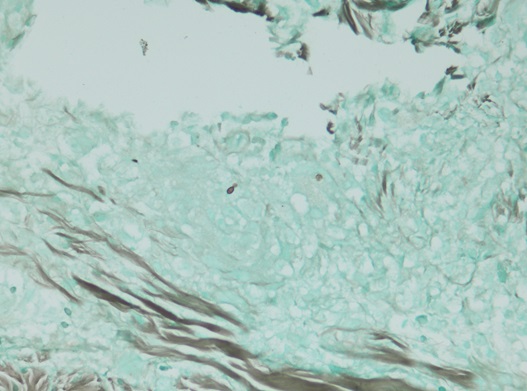
Figure 2. A Grocott stain highlights the presence of a budding fungal yeast. (x40 magnification).
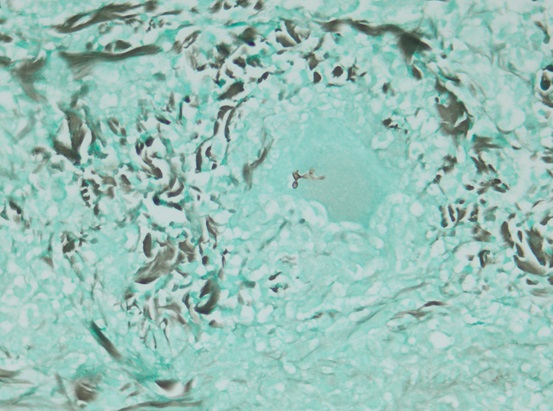
Figure 3. A Grocott stain highlights the presence of branching hyphae within a multinucleate giant cell. The hyphal form of sporothrix is rarely seen. (x40 magnification)
Culture results from a skin biopsy and a skin scraping were received confirming Sporothrix schenckii
Question 2: What risk factors predispose to sporotrichosis?
Answer to Q2
Sporotrichosis has traditionally been referred to as “gardeners’ disease”, particularly affecting those who cultivate roses. It is regarded as an occupational disease and individuals who work with wood, plants, flowers or infected animals are at risk of contracting the infection. It is usually transmitted through the direct inoculation of the fungus into the skin. Other occupational and leisure activities that have been associated with sporotrichosis include farming, hunting, mining and fishing.
A 55-year-old man was referred from the Dermatology clinic with a diffuse rash. Towards the end of 2013, he noticed subcutaneous lumps over his left upper arm and back, which gradually ruptured through the skin to form scaly ulcers. Some of the lesions were occasionally associated with a purulent discharge. Over the next few months, more lesions developed, now involving his face and legs. Of note, a lesion appeared on his nose, starting as a pimple., which gradually extended into the nasal cavity, eroding through cartilage. It was associated with a thick, purulent and, at times, bloody nasal discharge.
HIV infection may predispose to the development of invasive, atypical or disseminated sporotrichosis. The clinical picture varies according to the degree of immunosuppression: patients with preserved CD4 counts develop localized lesions from direct inoculation (similar to lesions in immunocompetent patients) while advanced HIV infection predisposes to disseminated lymphocutaneous or systemic extracutaneous disease.
Diabetes and alcoholism have both been described as risk factors, along with immunosuppression of any aetiology predisposing to disseminated or systemic disease.
Zoonotic transmission has been reported especially from domestic cats. Some cases have occurred in laboratory personnel working with cultures. Human-to-human transmission is rare.
Question 3: Discuss the laboratory investigation of Sporotrichosis
Answer to Q3
The diagnosis is based in the correlation of epidemiological, clinical and laboratory features. Clinical suspicion is required though usually the diagnosis is based on suggestive clinical features if patients present with classic lymphocutaneous sporotrichosis.
Culture: This is the gold standard for confirming the diagnosis of sporotrichosis. Aspirated material from a lesion, tissue biopsy samples, sputum or body fluids can be inoculated directly onto Sabouraud’s dextrose agar and incubated at room temperature. Growth may be noted within 5 days but can take a few weeks. In order to positively identify the organism as S. schenckii, dimorphism must be demonstrated by subculturing the fungus on an enriched media at 35-370C. This shows the fungal conversion to the yeast phase.
Histopathology: Special stains such as Gomori methenamine silver (GMS) and periodic acid-Schiff (PAS) are often used to enhance fungal detection. Sporothrix cells appear as oval to cigar-shaped and may have multiple buds. Organisms may however be difficult to visualize due to the paucity of yeasts in lesions. Tissue reaction to the organism manifests as mixed suppurative and granulomatous reaction in the dermis and subcutaneous tissue.
Serology: No serological tests have been shown to be useful in diagnosing sporotrichosis mainly due to low sensitivities and cross-reactivity
Molecular methods: Polymerase chain reaction techniques are showing promise but are limited to the research environment.
Question 4: What are the clinical syndromes of sporotrichosis?
Answer to Q4
Sporotrichosis is classified as a primary cutaneous disease or extracutaneous disease. The incubation period may vary from days to months.
Primary cutaneous disease
Lymphocutaneous: This is the most common form, commonly arising at sites of minor trauma and inoculation of the fungus into the skin. The initial lesions are papulonodular and can range in size from a few millimeters to a few centimeters. Lesions can be smooth or verrucous and often ulcerate. Secondary lesions arise proximally and follow lymphatic channels as they develop similarly to the initial lesion. The mucosal form is a variant of cutaneous disease where involvement of nasal mucosa or septum may cause bloody secretions. Mucosal lesions are often associated with pre-auricular and submandibular lymphadenopathy.
Fixed: This lesion forms a painless plaque and tends not to spread locally. The natural history is that of a chronic, non-healing ulcer over weeks or months.
Disseminated: Multiple skin lesions at non-contiguous sites without systemic spread characterize this form.
Extracutaneous disease
Extracutaneous disease is less common and more difficult to diagnose, though are now more frequent as a result of the HIV epidemic. Bone is most often affected with the osteoarticular form developing either by contiguous or haematogenous spread. This form can manifest as tenosynovitis, periostitis or monoarticular arthritis, most often involving major joints of the extremities. Most cases of osteoarticular Sporotrichosis follow cutaneous disease in immunocompromised patients, whereas primary disease is very rare.
Pulmonary disease may present with a productive cough, occasionally with haemoptysis, along with fever and weight loss. This is becoming increasingly common in AIDS, though it may also complicate alcoholism, chronic steroid use, chronic obstructive pulmonary disease and other immunosuppressed states. The clinical and radiological patterns (cavitary disease, tracheobronchial lymph nodes, nodular lesions) are similar to that of tuberculosis and may delay diagnosis.
Involvement of the central nervous system can occur as chronic meningitis or brain abscesses, though this is uncommon.
Visceral dissemination may occur in patients with HIV infection as evidenced by reports of liver and spleen involvement; fungemia with spread to GIT/ bone marrow/ lymph node sites; sinusitis with local invasion.
Question 5: Describe the management of sporotrichosis
Answer to Q5
The Infectious Diseases Society of America published guidelines on the treatment of sporotrichosis. Itraconazole at 200mg daily is the preferred option for cutaneous sporotrichosis due to its convenience and efficacy. The duration of therapy extends to 2-4 weeks beyond the resolution of all lesions, usually requiring 3 to 6 months for clinical cure. If relapse occurs after therapy is stopped, a higher dose of itraconazole at 200mg twice daily should be tried. However drug-drug interactions with antiretrovirals must be taken into account.
Susceptibility studies are not performed routinely and in vitro results may differ from the response noted in a clinical context. Fluconazole, voriconazole and micafungin have not shown adequate in vitro activity against S. schenckii. Posaconazole may show more in vitro activity than voriconazole, though clinical data is lacking.
Treatment of extracutaneous sporotrichosis is more difficult. Osteoarticular sporotrichosis requires itraconazole 200mg bd PO for at least a year with response being slow. Amphotericin B is the treatment of choice for pulmonary disease until a clinical response is noted, after which itraconazole can be given orally for up to a year. Amphotericin B is also recommended as initial therapy for other forms of extracutaneous disease followed by itraconazole as maintenance therapy. In HIV infected patients, relapses and disseminated infections are common and chronic suppressive itraconazole therapy may be required.
The following table from the IDSA 2007 Clinical Practice Guideline summarises the treatment recommendations:
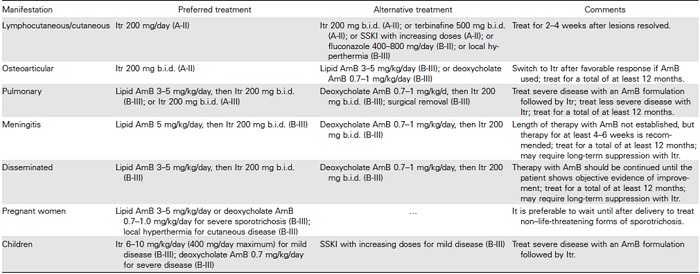
The patient was commenced on itraconazole 200mg daily and was discharged via the antiretroviral clinic where he was started on emtricitabine/ tenofovir/ efavirenz. His skin lesions were resolving slowly while he continued to work as a chainsaw instructor in wooded areas until he was lost to follow-up.
References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®