
Norma Bosman, Nelesh P Govender
An 11-year-old boy presented to the paediatric oncology outpatient clinic on 1 September 2014 with fever and back pain.
He was known to the clinic, and had been previously diagnosed with acute lymphoblastic leukaemia (ALL) in 2006.He had been in remission and off treatment since December 2009, but later relapsed in January 2012, and was restarted on chemotherapy.
He was admitted and started on a combination of IV piperacillin-tazobactam, amikacin and vancomycin. Laboratory samples, including blood culture, were submitted prior to starting antibiotics. Chemotherapy was discontinued temporarily. His admission neutrophil count was 2.9 x 109 cells/L (reference range: 1.40 – 5.20 x 109 cells/L).
An abdominal CT scan done 2 days later revealed a left renal abscess. Six months prior to this admission, the patient had had a pigtail catheter inserted for the drainage of an abscess in the same kidney. No pus samples had been submitted to the laboratory during the previous admission.
Question 1: What is the differential diagnosis of a renal abscess in an immune-compromised patient?
Answer to Q1
A renal abscess is an uncommon complication of a urinary tract infection (UTI) in immune-competent patients. It usually occurs secondary to obstruction of an infected kidney, occasionally occurs secondary to bacteraemia, but may also occur insidiously. The implicated bacterial pathogens are usually Gram-negative enteric bacteria, Gram-positive cocci and occasionally fungi, especially Candida species.
In immune-compromised hosts, however, the aetiology is different. Invasive fungal infections (IFI) remain an important cause of morbidity and mortality in leukaemia and transplant patients. For a long time, invasive aspergillosis was the predominant IFI in patients with haematological malignancies. More recently, there have been increasing reports of unusual and more difficult-to-treat moulds such as Mucorales, Fusarium species, and Phaeohyphomycetes1.
Admission and subsequent blood cultures submitted to the laboratory remained negative.
Eight days later, the patient was taken to theatre, and a left nephrectomy was performed. Pus from the abscess was submitted to the clinical microbiology laboratory for bacterial and fungal MC&S, and a tissue sample was submitted to histopathology.
Within 48 hours of incubation, a mould was isolated from the pus.
Preliminary microscopy results from histopathological examination showed large areas of “geographic necrosis” within the renal parenchyma. “Broad, septate hyphae which show branching at acute angles” were also observed within the areas of necrosis. Features of an ascending pyelonephritis, with pus casts in the collecting ducts, as well as an acute purulent interstitial nephritis with micro-abscess formation were also seen.
Question 2: What are the likely fungal pathogens?
Answer to Q2
Moulds belonging to the genera Aspergillus, Fusarium and Scedosporium all typically appear in histological tissue sections as septate hyphae (usually narrow width) with branching at acute angles. In contrast, moulds within the order Mucorales tend to produce broader, ribbon-like hyphae with few or no septa and branch at right angles. However, it is not always possible to distinguish these two groups by histological examination alone. It has been observed that the prevalence of Aspergillus infections, although still common, has decreased significantly in the last 5 years whereas the frequency of the Mucorales infections has increased slightly1.
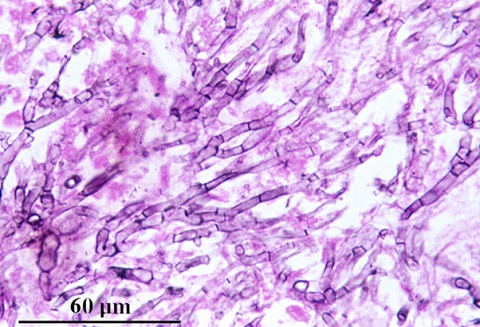
Figure 1: Grocott’s methenamine silver (GMS) stained tissue section of lung showing dichotomously branched, septate hyphae of Aspergillus fumigatus. [Source: Kaminski’s Digital Image Library of Medical Mycology; available from www.mycology.adelaide.edu.au]
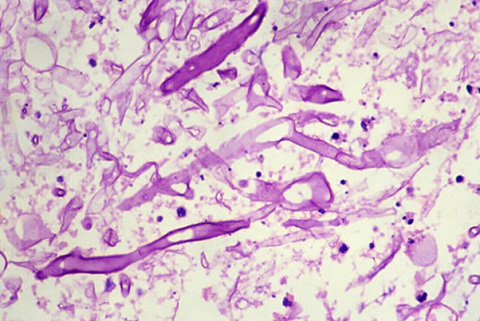
Figure 2: Haematoxylin and eosin (H&E) stained section of lung tissue showing the broad, infrequently septate, thin-walled hyphae of Absidia corymbifera. [Source: Kaminski’s Digital Image Library of Medical Mycology; available from www.mycology.adelaide.edu.au]
The mould was identified in the microbiology laboratory as Aspergillus and voriconazole was advised for targeted treatment. Due to initial unavailability of voriconazole, the patient was started on amphotericin B deoxycholate instead, and after 18 days changed to voriconazole. He recovered well post-operatively, and was discharged home a month later to continue voriconazole and chemotherapy.
Question 3: How common is renal aspergillosis?
Answer to Q3
Aspergillosis is an opportunistic infection caused by fungi of the genus Aspergillus. Clinical syndromes range from colonisation and localised allergic responses to the organism, to invasive infections involving, commonly the lungs, and any other organ systems in the body. Common predisposing factors include immune-compromised states such as underlying malignancy (including haematological malignancies), diabetes mellitus, renal or liver dysfunction, chronic obstructive pulmonary disease, corticosteroids and chemotherapy and stem-cell and solid organ transplantation 2.
Aspergillosis limited to the urinary tract and not occurring as part of disseminated infection is rare, although a few case reports have been described in the literature affecting patients with haematological malignancies, as well as patients with AIDS2,3,4. Its pathogenesis may involve ascending infection from the lower tract, haematogenous renal involvement, or secondary to aspergillosis of the renal pelvis from calculus formation. The most common is from haematogenous spread leading to abscess formation 2.
Patients may present in renal failure, with a renal mass or perinephric abscess, ureteric obstruction, haematuria, ±non-specific symptoms such as fever and flank pain.
In an autopsy study of IFI in patients with haematological malignancy conducted over a period of 20 years, Aspergillus spp. accounted for the majority of infections, even though a decline in the number of cases was noted during this period 1. The species identified included A. flavus, A. terreus, A. niger, and A. fumigatus. Of these, the percentage of infections attributable to A. fumigatus was found to have increased over the study period. In addition, Aspergillus infections, most frequently affected the lung (92%), the central nervous system (25%), heart (24%), kidney (15%) and the gastrointestinal tract (15%) 1.
Question 4: What is the recommended treatment for renal aspergillosis?
Answer to Q4
Voriconazole is recommended for the primary treatment of invasive aspergillosis. Although most of the evidence and data have been obtained from patients with invasive pulmonary aspergillosis, there is enough experience to recommend this agent for the treatment of extra-pulmonary and disseminated infection5.
Voriconazole has been shown to be superior to deoxycholate amphotericin B (D-AMB) as primary treatment of invasive aspergillosis, however, liposomal amphotericin B (L-AMB) can be considered as an alternative in some patients 5.
There are limited data on the management of renal aspergillosis. Although medical management may be successful in the treatment of small abscesses, surgical drainage or nephrectomy may be required for larger abscesses 5. Prolonged antifungal therapy may also be required 2,3,4.
A few weeks later, the patient presented to the local hospital in septic shock. He was admitted to the intensive care unit (ICU), with plans to transfer him to the academic hospital the next day, but he demised during the night.
References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®