

She was initially treated with doxycycline and telithromycin . The malaria smear was negative and, as the antigen test for Plasmodium falciparum was positive, the Coartem ® was continued.
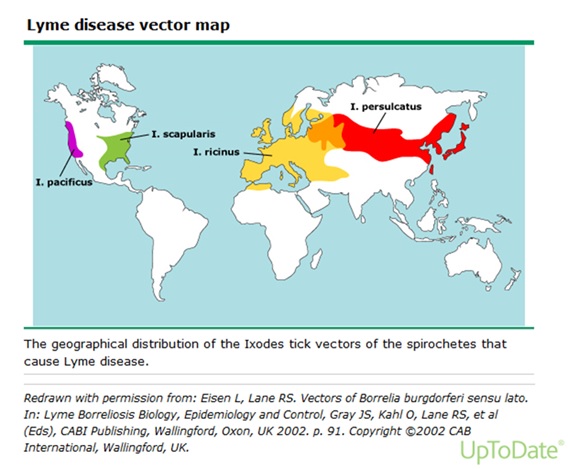
Question 5 - What is the aetiology and epidemiology/geographical distribution of Lyme disease?
Question 6 - What are the clinical manifestations of Lyme Disease?
Question 8 - What is the treatment of Lyme Disease?
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®