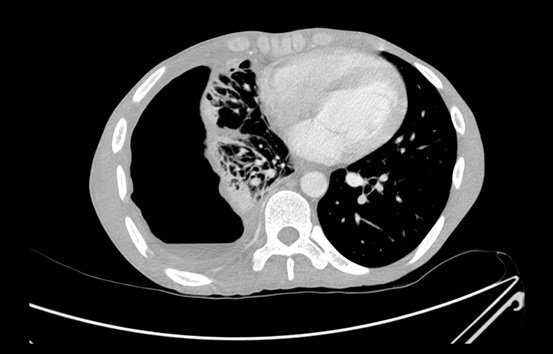
Question 2: An ‘empyema’ that looks like this is virtually pathognomonic for which diagnosis?
Answer to Q2
The pleural fluid shown has the appearance of “anchovy paste”, and this is virtually pathognomonic for amoebiasis.
The “anchovy paste” appearance is the result of a combination of necrotic and apoptotic material, and haemolysis of red cells that have bled into the cavity.
Question 3: Which is the most appropriate diagnostic test that can be performed to confirm this diagnosis?
Answer to Q3
The most appropriate diagnostic test at this stage would be serology for amoebiasis.
More than 95% of both amoebic liver abscesses and thoracic amoebiasis develop detectable antibodies. Such testing may be performed by indirect haemagglutination assays (IHA) or ELISA assays .
Microscopy may demonstrate trophozoites from aspirated material, but sensitivity is poor.
Antigen testing and molecular diagnostics (PCR) on aspirated material are both highly sensitive and, especially in the case of PCR, highly specific. However, they are expensive and generally limited to reference laboratories in Southern Africa. In the context of this case, they would be unlikely to add anything to serology, which is much cheaper and more readily available.
Question 4: Primary amoebic empyemas are very rare. Where else should one look in the body to see if there is another (primary) focus of infection?
Answer to Q4The abdomen should be scanned to look for a ruptured amoebic liver abscess. Almost all amoebic empyemas are the result of such an event1.
Although both an abdominal ultrasound and a contrasted abdominal CT scan were initially reported as normal, alert infectious diseases doctors insisted on a review of the scans.