
Buhle Makongwana, Helena Rabie and Mark Cotton
An 8-month old infant presented with 3-day history of:
10 days prior he had a cold
He was not HIV exposed but had a history of a tuberculosis contact.
On clinical assessment:
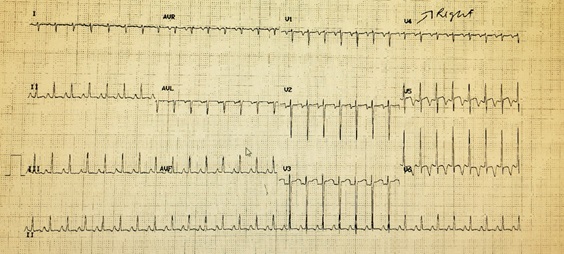
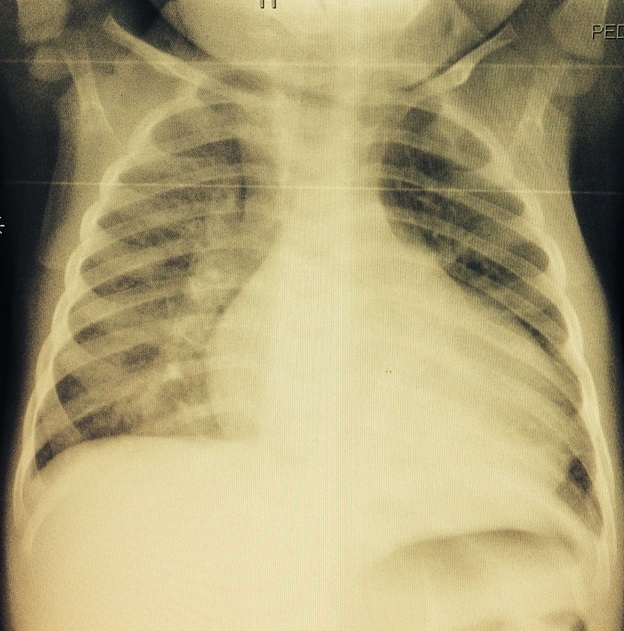
Figure 2: The CXR showed: pulmonary infiltrates with a slightly increased cardiothoracic ratio
The transthoracic ECHO-cardiogram confirmed severe left ventricular dysfunction dilation with an ejection fraction of less than 20 with moderate mitral and tricuspid regurgitation.
Question 1: What is the most likely cause of this child’s acute cardiac dysfunction?
Answer to Q1
The most likely cause is a fulminant myocarditis probably due to a viral infection.
Acute myocarditis is a condition resulting from inflammation of the myocardium. Although there are a number of causes including infectious, post infectious, toxic and systemic disorders in children the condition is usually due to infection. 1,2,4,5
Disease occurs sporadically or in epidemics.8,9
There is a lack of good data on the incidence and prevalence of myocarditis worldwide due to the variability of clinical presentation from asymptomatic to a sudden catastrophic event and dilated cardiomyopathy.
A bimodal age distribution is reported with the first peak from 6-12 months and the second around 16 years. In a children younger than 12 years the male to female ratio is 1:1 however the disease is more common in males after 12 years of age.2,8,10,17
A retrospective study in Canada estimated prevalence of myocarditis presenting to their emergency department was 0.5 cases per 10,000 visits other reports suggesting 1 per 100,000 children. 8,9
There is very little local data to delineating the demographic information, incidence, prevalence causes and outcomes of children with myocarditis but in 2014, 8 children died of suspected or confirmed myocarditis at a single South African center (personal communication H Rabie)
Diagnosis can be challenging:
Question 2: Which viruses cause acute viral myocarditis?
Answer to Q2
Enteroviruses, adenovirus, (commonly types 2 and 5) parvovirus B19, and human herpes 6 (HHV-6) have been noted to be particularly important causes of viral myocarditis but influenza, hepatitis A and a host of other viruses have been associated with viral myocaritis. 1,2 In high resource settings there seems to be a shift in the potential viral causes of myocarditis. In the past in the United States, entero - and adenoviruses were the most common causes of viral myocarditis.
Recently the trend has shifted to parvovirus and herpes virus.8,9 After 1995, the prevalence of enterovirus decreased and the prevalence of adenovirus increased however more recently, Parvovirus B19 has been reported as the most commonly detected viral genome. In one study of myocarditis a 72% prevalence of Parvovirus B19 illustrates this interesting trend in the changing epidemiology of viral myocarditis over the past few decades. Whereas the pathogenic role of enterovirus and adenovirus in myocarditis is well established, the role of Parvovirus B19 is uncertain. It still needs to be establishes whether it is an incidental or pathogenic agent in myocarditis.17
Question 3: How can the diagnosis of myocarditis be confirmed?
Answer to Q3
Endomyocardial biopsy is considered the gold standard for the diagnosis of myocarditis.16 The specimen is evaluated with light microscopy according to the Dallas criteria. Adding immunohistochemistry and viral genome analysis now enhances this traditional method. When using the traditional assessment only the sensitivity is low in pediatric myocarditis patients due to sampling error and the focal and transient nature of the infiltrate and necrosis.
Locally biopsies are rarely performed due to the potential risk, other noninvasive methods are used including cardiac MRI where possible.3
Swabs from rectal and nasal mucosa should be cultured for viruses and PCR performed. The results of viral identification from tracheal aspirates by PCR have been shown to correlate well with those obtained from myocardium and the lower respiratory tract.
In the absence of positive viral cultures and pcr, acute and convalescent antibody titers can be helpful in the diagnosis of a specific viral infection, a 4 fold increase in title should be shown to indicate causality.
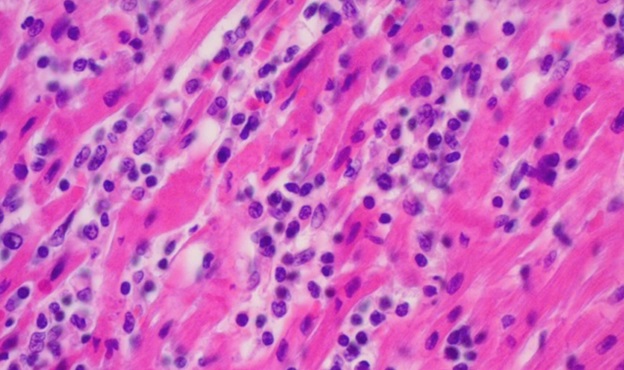
Figure 3: This post mortem photograph illustrates the lymphocytic infiltrate and necrosis seen in acute viral myocarditis
In our patient the PCR was positive for enterovirus.
Question 4: What are the some of the syndromes associated with enteroviruses?
Answer to Q4
Common to all is fever, irritability, lethargy, anorexia and rash. Most cases are mild but serious complications include sepsis, meningoencephalitis pneumonia, hepatitis, coagulopathy and enteroviral sepsis syndrome can occur. Post-infectious inflammatory diseases such as ADEM is also well recognized.
Question 5: What are methods of diagnosing enteroviruses?
Answer to Q5
Traditionally it has been viral isolation followed by immunofluorescent staining to detect cytopathic effects with the use of antisera, which allow identification of the infecting serotype. Highest yields are with samples from throat or nasopharyngeal swabs, rectal and stool samples and cerebrospinal fluid.
Serology relying on the detection of IgM or detection is rise of IgG is less useful and requires paired sera to be repeated in 2-3 weeks. Serology has good specify with poor sensitivity as there is no universal test against all the enteroviruses.
PCR methods are now widely used with good specificity and sensitivity whilst also yielding rapid results. PCR can be from throat swabs, nasopharyngeal aspirates, stools or rectal swabs. The yield from blood is usually low except in the setting of viraemia. Urine samples have a relatively low yield. 2,13,15
Tissue culture has limitations of expense and cannot grow all types of coxsackie virus due to wide variability within the enterovirus group. Growth in culture is also slow, up to 8 days.
Question 6: Is there any specific precaution to be taken from the basis of hospital infection prevention and control?
Answer to Q6
Enteroviruses are resistant to alcohol.
Question 7: What is the treatment of suspected viral myocarditis
Answer to Q7
Supportive care is the main stay of therapy.
Myocarditis is the result of both the infection and the inflammatory response. Immune modulation in the form of immune-suppression, intravenous immune globulin and corticosteroids has been used13.
Despite steroid use yielding conflicting results in adults, the effects have been favorable in some studies in children with active myocarditis. Prospective studies are however limited to a single small randomized controlled trial comparing 3 different immunosuppressive treatment strategies including a “steroid only” arm.25 This study failed to show any haemodynamic or clinical improvement with steroid use alone. A Cochrane review does not support the role of corticosteroids in the treatment of myocarditis.29
Intravenous immunoglobulin (IVIG) is the most commonly used immune modulator in myocarditis.
Intravenous immunoglobulin (IVIG) is the most commonly used immune modulator in myocarditis. Robinson et al conducted a multi-database search including patients of all ages with myocarditis treated with IVIG. They concluded that if there is evidence that ongoing, active infection may be causing persistent cardiac dysfunction, IVIG may be helpful. Drucker et al showed a statistically significant improvement in survival in paediatric myocarditis patients treated with high-dose IVIG and this is echoed by Saji et al, who found improved recovery of LV function and a tendency for better survival during the first year after presentation2,27,28,29. A Cochrane Database compared IVIG-treated patients and non-IVIG-treated patients, and found similar outcomes including the incidence of death, the need for heart transplantation and the replacement of an LV assist device in the acute phase, improvement in LVEF, and functional capacity as assessed by peak oxygen consumption after 12 months.29. However many patients with myocarditis have spontaneous improvement. It is therefore difficult to know if the observed improvement after treatment with IVIG is attributable to treatment versus the natural course of the disease.
The rationale use of antiviral drugs results from the knowledge that most common causes of myocarditis are induced by viral infections. Acyclovir and ganciclovir may be considered in patients with herpes virus or cytomegalovirus infections but there is no approved anti-viral treatment for the treatment of enteroviral infections. Two viral capsid inhibitors pleconaril and popcapavir have been used in studies of complex and in selected cases.13,24 Children with severe Entrovirus 71 disease may have a better outcome if treated with milrinone, a phosphodiesterase 3 inhibitor.
Reference
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®