
Harhsa Lochan and Brian Eley, Paediatric Infectious Diseases Unit, Red Cross War Memorial Children’s Hospital, and the Department of Paediatrics and Child Health, University of Cape Town
A 2-month old boy presented with a 2-week history of cough, fever and respiratory distress requiring admission to a level 2 hospital. He was born at term and there no complications in the immediate post-natal period.
Past medical history included 2 previous episodes of bronchiolitis, the most recent 11 days prior to this admission. There was no history of TB or HIV exposure, failure to thrive or dysmorphic features noticed.
On presentation, he was hypoxic with oxygen saturation of 91% in room air. There was also extensive oral candidiasis. The chest radiograph showed right upper lobe consolidation (Figure 1). He was transferred to a level 1 facility on day 1 of the current illness where he completed 7 days of antibiotics (ampicillin and gentamicin initially). Blood culture was negative after 5 days of incubation and there were no viruses detected on the nasopharyngeal aspirate PCR.
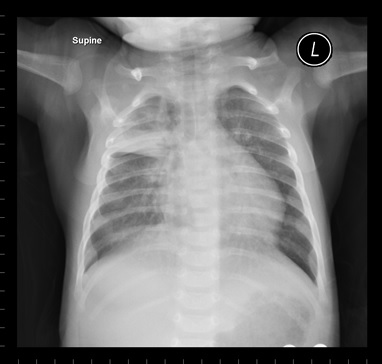
Figure 1
Despite antimicrobial and oxygen therapy, there was minimal clinical improvement. Ten days into the current illness, he was transferred to a level 3 hospital from the level 1 facility. Continuous positive airway pressure (CPAP) ventilation was commenced. Ertapenem was also initiated for a presumed nosocomial infection.
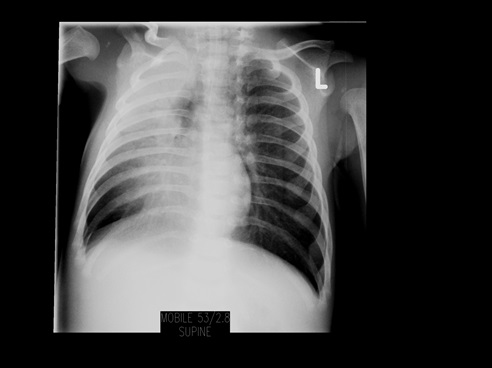
He continued to have ongoing respiratory distress with a respiratory rate up to 100 breaths/min, marked subcostal and intercostal recession and persistently high temperatures up to 38.1°. The chest radiograph showed persistent RUL consolidation (Figure 2) despite appropriate antibiotics which included clarithromycin to treat for possible mycoplasma or chlamydial infection. There was no history of aspiration during the admission.
The following were relevant investigations performed during the course of the infant’s admission to hospital:
Bocavirus was detected on a repeat nasophayngeal aspirate PCR. The HIV rapid test was negative. The patient was screened for tuberculosis and induced sputum specimens were Xpert MTB/RIF and culture positive for Mycobacterium tuberculosis complex, rifampicin susceptible. The CMV viral load was raised at 7561900 copies/ml (log >6.70).
Question 1: What is the differential diagnosis for a child with a persistent pneumonia at a single site and unremitting fever?
Answer to Q1
The definition of persistent pneumonia is the continuation of symptoms and radiographic findings beyond 4 weeks after onset. In adults and children with community acquired pneumonia, radiological abnormalities lag behind clinical resolution.
Possible causes of a persistent or progressive pneumonia at a single anatomical site could be differentiated into pathogen-related or host-related causes due to congenital or acquired anatomical abnormalities.
Pathogen-related causes:
Host-related causes could be due to:
Possible causes of a persistent or recurrent pneumonia:
Question 2: How do you interpret the results of the white cell count and the differential count and the significance thereof?
Answer to Q2
The total white cell count was within the age-specific reference range with a marked elevation at day 10 post-admission. What is striking is the persistently low absolute lymphocyte count. In children a normal lymphocyte count is usually >3 x 109/l.
Lymphopaenia could be caused by severe viral, bacterial or fungal infections, HIV infection, steroid therapy or primary immunodeficiency affecting lymphocyte production and development.
Answer to Q3
Due to the persistent lymphopaenia, this patient should have lymphocyte subpopulations analysis and total immunoglobulin levels performed to exclude a primary immunodeficiency.
The patient’s results were as follows:
IgG 2.67 g/l (normal 3-10)
IgA < 0.25 g />l (normal 0.1-0.7)
IgM < 0.25 g />l (normal 0.2-1.1)
Lymphocyte subset analysis:
The results show virtually absent T cells and NK cells. The B cells are also low spectrum of normal as evident by the low immunoglobulin levels.
Question 4: What is the likely diagnosis?
Answer to Q4
The blood results are compatible with a diagnosis of a primary immunodeficiency: severe combined immunodeficiency (SCID). This is in keeping with the B+T- NK+ phenotype of SCID which is X-linked in inheritance pattern.
Question 5: How do you interpret the Xpert MTB/RIF and sputum culture result?
Answer to Q5
The Xpert MTB/RIF is a molecular test that detects Mycobacterium tuberculosis complex.
Further molecular testing (PCR) of the cultured specimen differentiated the Mycobacterium complex to be that of vaccine M. bovis BCG species. Members of the Mycobacterium tuberculosis complex detected by the assay include Mycobacterium tuberculosis, Mycobacterium bovis, Mycobacterium bovis Bacillus Calmette-Guerin, Mycobacterium africanum, Mycobacterium canetti, and Mycobacterium microti. The other species within the Mycobacterium tuberculosis complex (Mycobacterium bovis subspecies caprae and Mycobacterium pinnepedi) have not been tested using the assay.
Patient Outcome and Discussion
The patient was isolated in a single cubicle, and strict contact precautions were instituted and enforced for all medical and nursing staff. Visitation was restricted to the parents. All procedures were performed using aseptic technique and sterile feeds were administered enterally. Intravenous immunglobulin (IVIG) was administered weekly during the course of his illness. He was treated for presumed infection with Pneumocystis jirovecii, CMV associated pneumonia, oral candiadiasis as well as disseminated BCG disease with rifampicin, isoniazid, ethambutol and levofloxacin. He underwent evaluation for a bone marrow transplant.
Primary immunodeficiencies are a rare group of disorders that affect the development, ± function of the immune system.
It should be suspected in children in whom:
Secondary immunodeficiencies occur much more commonly than primary deficiencies.
Transient periods of immunosuppression have been associated with viral infections such as measles, influenza virus and CMV. These infections can induce lymphopaenia and T-cell anergy which are less severe in their manifestations. The bone marrow could also be infected with bacterial and viral infections that cause pancytopenia and predispose immunocompromised patients to infections.
Other common causes of secondary immunodeficiency include:
Severe combined immunodeficiency (SCID) is a group of genetic conditions characterised by profound deficiencies in peripheral T-cell numbers and function. In some types B-cells, natural killer cells or both may also be deficient. Severe T-cell deficiencies compromises B-cell function even if present in normal numbers.
SCID defects are classified according to the immunological phenotype:
Clinical presentation
The infant with SCID presents early in life with bacterial, viral or fungal infections. Clinical presentation is similar regardless of the immunological phenotype. Infections usually involve the respiratory and gastrointestinal tract. Chronic diarrhoea may lead to failure to thrive. Pneumonia is commonly due to infection with Pneumocystis jiroveci as well as cytomegalovirus, adenovirus, respiratory syncitial virus or parainfluenza type 3 virus. Other fungal infections can manifest with severe mucocutaneous candidiasis. Skin rash, in the form of chronic eczema or generalised exfoliative erythroderma, might reflect graft-versus-host disease caused by maternal T-cell engraftment in infants with SCID. Children who have received BCG at birth are at risk for dissemination. Adenosine deaminase deficiency patients may also present with deafness, costochondral abnormalities, neurological impairment and liver toxicity.
Diagnosis
The diagnosis of SCID is considered a clinical emergency. The majority of patients will present by six months of age.
Blood tests to aid in the diagnosis:
Management
The principles of management include:
Haematopoietic stem cell transplant offers a cure of SCID. HLA-identical matched sibling or family donor HSCT is recommended and offers >90% survival. HSCT from HLA-mismatched related donors provides good results when performed in the first 3 ½ months of life.
References:
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®