
Linda van der Westhuizen: Mediclinic Southern Africa
Briette du Toit
A previously healthy 39 year old female residing in the Western Cape was admitted to the Emergency Centre on the 5/1/2014. During the period 25 -29 December 2013 she had travelled to numerous farms in the Wepener district in the Free State and participated in farming activities that included hiking and hunting. On admission she presented with a history of severe headache, low grade fever and neck stiffness since 29/12/2013, when she was admitted and treated for meningitis in another healthcare facility until her discharge on the 1/1/2014.
Shortly after her discharge on the 1st of January, she found a tick in her navel and went to her general practitioner on the 2/1/2013 with symptoms of a persisting low grade headache and malaise. No skin rash or eschar was observed at the bite site. Doxycycline was prescribed. On 4/01/2014 a very fine rash appeared and covered her whole body. During the night of the 4th of January her condition deteriorated. She presented with diarrhoea and vomiting. Her family reported that she was confused and not able to have a meaningful conversation. At 17h00 on 5/01/2014 she vomited macroscopic blood and lost consciousness for a short period of time.
On arrival to the Emergency Centre she was awake and appeared oriented when spoken to. The triage nurse alerted the professional nurse about the patient’s condition as soon as she was told about the tick bite. An intravenous line was inserted and no excessive bleeding was observed at the puncture site. During consultation it was found that she had a severe headache and had been taking large doses of NSAID and other oral “over the counter” analgesia since the 29/1/2014. She had a small amount of blood in her sputum and her gums appeared to have a minimal amount of petichiae. No active bleeding was observed. Bloods were drawn for:
Haematology:
Chemistry:
She was admitted into the General ICU. On 6/1/2014 her left arm became oedematous and she developed a large haematoma around the intravenous puncture site, but no active bleeding was observed. At 14H00 she started with severe projectile haematemesis and was moved to an isolation room. A grand mal seizure at 17h45 caused her neurological status to fluctuate between non-responsive, extremely agitated, restless and confused with severe whining. Her skin colour changed to grey-blue and she developed melena stools.
Intra-cerebral haemorrhage was ruled out with a CT scan, but her neurological status deteriorated during the night. In the early hours of 7/1/2014 she pulled out her intravenous line and uncontrolled bleeding occurred at the puncture site. The situation deteriorated and all puncture sites made by the haemolances to obtain blood samples for HGT and HB started to bleed. The first signs of epistaxis were observed at 06h50. Her cardiovascular status became unstable with an atrial fibrillation of 210 -220 b/min, hypotension and saturation of 66% on face mask oxygen. She was intubated and ventilated at 10h10; a CVP and arterial line were inserted to assist in the cardiovascular monitoring and support.
Isolation for viral haemorrhagic fevers (VHF) was implemented on the 7/1/2014 at 13h00. On the 8/1/2014 a positive CCHF RT-PCR was received from the National Institute for Communicable Diseases (NICD). She developed all the classic signs of CCHF that included haematuria, vaginal bleeding, tachycardia, sever ecchymoses, hepatomegaly, splenomegaly and a persistent uncontrolled pyrexia of 38-43°C. On the 10/1/2014 the blood chemistry indicated a MDRD 7, creatinine of 652 and urea of 61.9. Dialysis was commenced on the 10/1/2014. Numerous blood products were administered on several occasions.
Multiple interventions done by the multidisciplinary team ensured that she gradually improved haemodynamically. Due to severe abdominal pain and discomfort surgical intervention for severe ascitis was needed. She was transferred out of the initial isolation area created in the General ICU to an isolation area in the surgical ward and discharged on the18th of February 2014.
The patient was discharged after spending 6 weeks in hospital; she was readmitted for severe peritonitis and pyrexia due to abscess formation. She is currently progressing well. No secondary cases were reported, despite the delay in the correct diagnosis and the late implementation of precautions for VHF.
Question 1: What are the important differential diagnoses?
Answer to Q1
1. Viral haemorrhagic fever
Viral haemorrhagic fever (VHF) is a general term for a severe illness, often associated with bleeding, that may be caused by a number of RNA viruses belonging to four different viral families (Table 1). Humans may acquire infection through contact with blood and tissues of a viraemic animal, another human case or through the bite of an infected tick. Rift Valley Fever and Crimean Congo haemorrhagic fever (CCHF) are endemic to South Africa. CCHF in South Africa is transmitted by ticks of the Hyaloma species such as bont-poot bosluis (striped leg tick). The incubation period varies from 2 to 21 days. Although the clinical presentations may vary, there are some common features of the initial disease manifestation that are similar and include high fever, malaise, myalgia, headache and abdominal pain. As the disease progresses the patient may present with vomiting, mucosal (including gastrointestinal) bleeding, altered mental state, skin rashes, oedema, and hypotension.
Blood for VHF testing should be submitted to the Special Pathogen Unit at the National Institute of Communicable Diseases (NICD), the only place in South Africa where the tests are performed. A diagnosis of CCHF is confirmed by reverse transcription polymerase chain reaction assay and by the presence of CCHF virus-specific IgG and IgM antibodies detected by enzyme-linked immunosorbent assay. Other clinical features include leucopoenia, thrombocytopenia, abnormal PT and PTT and raised AST and ASL.
Nosocomial transmission in healthcare facilities has been reported and that is usually due to non-compliance to standard and transmission based precautions while caring for affected patients.
According to the NICD, CCHF cases occur sporadically in South Africa, with an average of five cases per year. Since the first recorded case in 1981, 192 cases of CCHF have been recorded in South Africa. Most cases that were reported in the past were single, isolated episode. The only recorded outbreak of CCHF virus in humans in Africa occurred in 1996, with 17 cases diagnosed at an ostrich abattoir in Oudtshoorn in the Western Cape Province. The majority of these cases were exposed to ticks via tick bites or squashing of ticks; the remainder were assumed to have been infected by exposure to infected ostrich tissues or blood whilst removing feathers and hides.
From January 2000 to August 2013 fifty-four cases of CCHF were laboratory-confirmed in patients from South Africa. The overall mortality rate during this period was 35% (19 deaths). CCHF cases have been recorded in all nine provinces of South Africa, with the majority of cases occurring in farming areas in the Northern Cape (n=20) and Free State (n=17) provinces. In 2013 five cases of CCHF were reported in South Africa and one case to date in 2014.
Table 1: Common viral causes of haemorrhagic fever
The other viral haemorrhagic fevers do not normally occur in South Africa and since the case presented here did not travelled outside the borders of South Africa, Ebola, Lassa and Marburg would not normally be considered in the differential diagnosis. However imported cases (through cross-border trafficking of patients) have been described and have been responsible for nosocomial outbreaks. The history of travel and hunting is an important clue, especially in the Free State province where a high incidence of CCHF is seen. In addition there is the possible risk of exposure to blood and tissue of animals where there is a history of hunting. The presentation with a prodromal illness preceding the bleeding is fairly typical of CCHF, as are the laboratory findings of thrombocytopaenia, leucopenia and elevated transaminases. This patient was in fact confirmed to have Crimean-Congo haemorrhagic fever.
2. Tick bite fever (Rickettsial infection)
Probably the two commonest causes of tick bite fever in South Africa are Rickettsia conorii and Rickettsia africae. The infection is spread by the bite of Amblyomma ticks, and usually occurs after exposure in a rural environment. Fever and headache are important clinical features and in R. africae infection, an eschar is almost always present. Although a rash is an important clue, it may not be present in all cases. This differential diagnosis should be considered in such a case given the travel history and possible tick exposure; however the absence of an eschar makes this diagnosis less likely.
3. Meningococcal infections
Meningococcemia can present with fulminant sepsis, fever, hypotension, thrombocytopaenia with haemorrhage, and ecchymoses. According to data from the NICD, 233 cases of invasive meningococcal disease were reported in South Africa in 2013.
Neisseria meningitidis is spread primarily by the droplet route, and close household contacts of cases are at an approximately 400 fold increased risk of developing symptomatic infection. This is probably due to a combination of shared environmental factors (e.g. smoking), possibly genetic factors, and transmission of the organism from asymptomatic carriers. However, spontaneous community cases still account for the vast majority of meningococcal disease, thus the absence of a history of exposure by no means rules the condition out.
4. Severe bacterial sepsis
Severe bacterial sepsis, usually Gram negative, can also present with fever and a DIC (disseminated intravascular coagulation), which may result in haemorrhagic manifestations. Any patient presenting with a fever and potential DIC should have blood cultures taken and be started on an antibiotic with Gram negative cover (such as a 3rd generation cephalosporin).
Answer to Q2
Guinea in West Africa is currently experiencing an outbreak of Ebola virus disease (EVD), formerly known as Ebola haemorrhagic fever. It is suspected that the outbreak has spread to Liberia. This is the first recorded outbreak of EVD in these Western African countries, where Lassa fever is commonly reported. This outbreak began in early February 2014, and laboratory studies demonstrated that Zaire Ebola virus is the virus responsible for the outbreak. This is a highly virulent virus with a case fatality rate of up to 90% reported in previous outbreaks.
On the 25th of April, the World Health Organisation (WHO) reported a cumulative total of 218 clinical cases of EVD in Guinea, including 141 deaths. To date, 191 patients have been tested for EVD infection and 115 cases have been laboratory confirmed, including 72 deaths. In addition, 42 cases (34 deaths) meet the probable case definition for EVD and 61 cases (35 deaths) are classified as suspected cases. Twenty-six (26) health care workers (HCW) have been affected (18 confirmed), with 16 deaths (12 confirmed). The median age of 198 clinical cases for whom the age is known, is 35 years; the age breakdown is as follows: 0-9 years (11%), 20-59 years (72%) and ≥60 years (11%). From the 13th of March to date 35 clinical compatible cases of EVD were reported in Liberia; 6 confirmed cases, 2 probable cases and 27 suspected cases.
The ecology of the Ebola virus is not completely understood, but it is believed that the infection is transmitted by direct contact with blood, body fluids and tissues of infected animals or people. Animals include chimpanzees, gorillas, bats, monkeys, forest antelope and porcupines, but the most likely reservoir of the virus includes specific species of arboreal bats, and contact with these animals and/or their excretions/secretions may also result in transmission of the virus to humans. Human-to-human transmission occurs in the community through direct contact with the blood, secretions, organs or other bodily fluids of infected people, and indirect contact from environmental contamination. Burial ceremonies in which mourners have direct contact with the body of the deceased can also play a role in the transmission of Ebola. HCWs have frequently been infected while treating patients with EVD. This has occurred through close contact with patients where IPC principles were not adhered to.
Severely ill patients require intensive supportive care. No specific treatment is available.
Risk of imported Ebola virus disease to South Africa
The risk of infection for travellers is very low since most human infections result from direct contact with the body fluids or secretions of infected patients, particularly in healthcare facilities due to the use of contaminated medical devices such as needles and syringes and unprotected exposure to contaminated body fluids.
Since the current outbreak is reported in countries and areas which are not frequented by many tourists or travellers, the risk of EVD cases being imported into South Africa is low. It is important however, that healthcare workers who were involved in the outbreak response team may present for medical care in South Africa. A high index of suspicion is important for such cases. A detailed history regarding travel and level of contact with suspected/confirmed EVD cases is extremely important.
The World Health Organization (WHO) does not recommend any travel or trade restrictions applied to West African countries, however; all requests for medical evacuation of persons from Guinea, Liberia, Sierra Leone or Mali with febrile illness or suspected infectious disease will need careful evaluation by the Port Health officials.
While the risk of introduction of Ebola virus into South Africa is considered low, we strongly recommend that surveillance for viral haemorrhagic fevers (and at present, particularly EVD), be strengthened. This should be done primarily through Port Health services, but it is also extremely important that public and private practitioners are on the alert for any ill persons that have travelled to viral haemorrhagic fever risk areas.
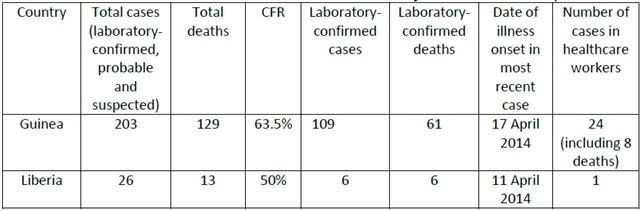
Table 2: Ebola virus disease outbreak in West Africa: summary of cases as at 17 April 2014
Question 3: What are the recommended infection prevention and control (IPC) precautions that needs to be implemented when managing a patient with a VHF?
Answer to Q3
What are the recommended infection prevention and control (IPC) precautions that needs to be implemented when managing a patient with a VHF?
In a previous case of the month, published in May 2011, the 9 key points of VHF (Viral Haemorrhagic Fever) Isolation Precautions” published by the World Health Organisation (WHO) in 1998 was discussed. The guideline was developed in order to limit outbreaks of VHF in healthcare facilities by preventing secondary cases of infection in health care facilities, and these have been adopted by the draft South African National Infection Control Policy, as follows:
1. The use of standard precautions in all patients
Standard precautions must be applied to all patients all the time. Standard precautions are designed to minimise exposure to blood and body fluids and mucous membranes by HCWs. It included the wearing of gloves and gowns when there is a risk of contact with blood or body fluids, as well as use of facial protection if splashes are likely. Other elements of standard precautions include safe waste disposal, safe disposal of sharps, hand hygiene and the wearing of appropriate personal protective equipment. After making a diagnosis of VHF, additional transmission based precautions, such as contact -, droplet- and airborne precautions (when procedures are performed where there is a risk of aerosolisation) must be implemented in addition to standard precautions.
2. Prompt identification of suspected cases of VHF
Due to the fact that the signs and symptoms of VHF are non-specific and similar to many other diseases, a diagnosis is often challenging. VHF may therefore not be suspected until the patient develops more advanced signs. If a patient has unexplained bleeding from mucus membranes (gum, nose, vagina), skin (puncture sites, petechiae), conjunctivae (red eyes) or gastro-intestinal system (vomiting blood, bloody or dark stools) associated with fever, and or shock, then the patient should be immediately isolated. HCW should have a high index of suspicion in VHF endemic areas and in non-endemic areas (especially if there is a history of travel). Additionally, a history of contact with someone with fever and bleeding should be treated as highly suspicious of VHF.
3. Immediate isolation of the suspected patient
4. Use personal protective equipment (PPE)
All health care workers, support staff (such as cleaners) and laboratory staff who provide direct patient care to suspected and confirmed VHF patients must wear adequate protective clothing before entering the isolation room.
Used PPE must be disposed of appropriately after handling the patient.
5. Appropriate decontamination of all reusable supplies and equipment is important if single-use items cannot be used.
It is preferred that single-used items that can be incinerated should be used. If equipment has to be re-used, the following should be done:
First clean the surfaces and then disinfect.
6. Safe disposal of waste
All contaminated waste generated during the care of a patient with VHF must be disposed of safely and should be incinerated.
7. Safe burial practices
Health care workers should be aware of the family’s cultural and religious beliefs in order to counsel them appropriately and explain why some cultural practices relating to burial may have to be forbidden, including touching, cleaning or ritual purification of the body.
Appropriate PPE must be worn at all times and the body sprayed with a freshly prepared 1:10 000 ppm hypochlorite solution.
8. Community education (in cases where there is a concern that the VHF may spread in the community)
Educate the affected community about VHF and its modes of transmission.
9. Monitoring of contacts
A list of contacts of the index case must be compiled and the contacts must be monitored. If any contacts are symptomatic, they should be isolated, and screened immediately. If they are asymptomatic, they should be monitored daily for 14 days after the last contact for the development of fever. If fever is documented, then they must be admitted, isolated and tested for the particular VHF
It is important to obtain a thorough history, with specific questions related to travel and possible animal (or other vector) exposure when patients with non-specific symptoms present at a healthcare-facility. If the patient is reporting a bleeding tendency, it will be even more important to obtain a thorough history. A high index of suspicion is always necessary in order to identify potential cases of VHF. Due to the non-specific nature of the symptoms, it can be confused with a number of other, more common conditions. Delayed diagnosis increases the chance of horisontal transmission in the health care setting. Standard precautions must be applied to all patients all the time, regardless of underlying disease.
References:
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®