
Dr Jeannine van Lochem, SASTM
A 59 year old male patient with hypertension who smoked for 40 years was admitted for a prostate biopsy in January 2012. This proved to be an adenocarcinoma with a Gleason score of 7. A chest X-ray (CXR) was ordered as part of his work-up, and an abnormal mass was seen in the left upper lung. The mass was vaguely circumscribed.
Question 1: What would be your differential diagnosis for this lesion be?
Answer to Q1
A CT scan was performed in January 2012
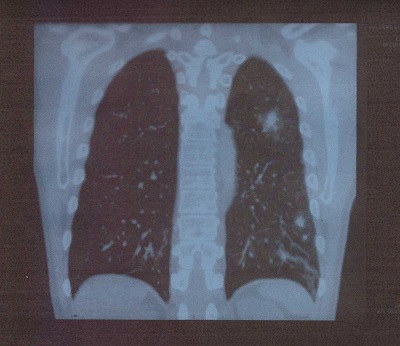
The mass was reported as potentially malignant on the CT-scan and a bronchoscopy and lung biopsy was done. Neither a frozen section or lymph nodes sent from theatre showed any sign of malignancy. Lymphnodes were reactive. A diagnosis of bronchopneumonia with abscess formation was made, and treated with antibiotics. The patient was discharged after five days. In March 2012 he underwent a radical prostatectomy and received radiotherapy afterwards.
He returned in September complaining of a dry cough. His prostate cancer was in remission. He was treated with clarithromycin, but his cough deteriorated over the next month. He developed a band-like chest pain, had occasional episodes of heamoptysis, but no fever or breathlessness.
Answer to Q2
The sputum cultured Moraxella catarrhalis. The chest X-ray showed a left lower lobe consolidation and a nodule in the anterior segment of the left upper lobe.
Blood abnormalities were:
The patient was given a two week course of moxifloxacin and remained well for one month.
Question 3: What are the risk factors for developing Moraxella catarrhalis pneumonia, what is the usual source, the typical clinicial presentations, and standard treatment?
Answer to Q3
Pneumonia due to M. catarrhalis is a marker for severe underlying lung disease and nearly half of patients die within three months of onset.
M. catarrhalis is a Gram-negative mucosal pathogen that is often found in the oropharynx of healthy people. Children have a much higher colonization rate than adults i.e. 76% vs. 4% in healthy and 10% in adults with COPD.1
In adults with chronic obstructive pulmonary disease, it can cause acute exacerbations. It can also cause pneumonia with or without a pleural effusion. However, only a small percentage of patients appear clinically ill.2
On CXR there is a lobar infiltrate in half of the cases, but there may be interstitial, segmental or diffuse involvement. It is also a common cause of otitis media in children and infants.2
M. catarrhalis is typically sensitive to macrolides, fluoroquinolones, tetracyclines and trimethoprim-sulfamethoxazole.
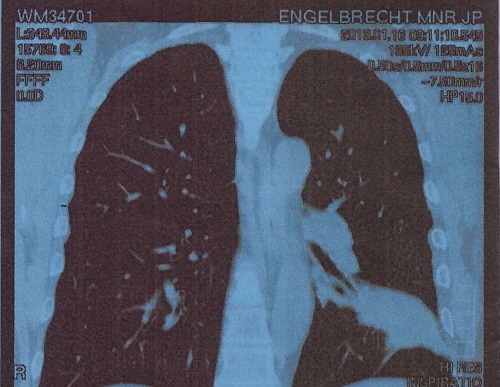
In January of 2013, he returned with left sided chest pain and severe haemoptysis. On CXR a dense opacity in the left lower lobe suggested a malignancy. The high resolution C/T scan showed a large solid spiculated mass with small central calcifications.
A bronchoscopy and thoracotomy was undertaken. A bronchial wash and frozen section was done which showed no malignancy. A diagnosis was made of pneumonia with a lymphocyte infiltrate and underlying bronchiectasis.
Question 4: What is bronchiectasis and what its major causes?
Answer to Q4
Bronchiectasis is the permanent and abnormal dilation of bronchi, either focal or diffuse. The normal bronchial tissue of cartilage, muscle and elastic tissue is replaced by fibrous tissue, which makes the airways more prone to bleeding. Causes include:
The patient was treated with intravenous antibiotics, bronchodilators and physiotherapy. The specialist reported though that, in the future, a lobectomy might be necessary.
He was seen again in April 2013 with symptoms of a chronic cough and a general sense of feeling unwell. A consultation with a pulmonologist was scheduled.
The pulmonologist ordered another CT scan and the mass on the left lower lobe again looked very suspicious of malignancy. He was booked for a left lower lobectomy.

Histology of the left lower lobe and a mediastinal lymph node was reported. Bronchiectasis was seen with colonies of Aspergillus fumigates and abscess formation. There were no signs of neoplasia or tuberculosis. Culture for tuberculosis after six weeks was also negative. The bronchial fluid from the lavage cultured an unidentified strain of Streptococcus.
Question 5: What is the epidemiology of aspergillosis, what conditions predispose to chronic pulmonary aspergillosis and how does it present?
Answer to Q5
Aspergillus fumigatus is a sacrophytic fungus that occurs naturally in the soil. Many people are in contact with it but only those with previous lung disease develop aspergillosis. It is found in immunocompetent as well as immunosuppressed patients and presents differently in each group. There are five patterns of chronic pulmonary aspergillosis:
Predisposing conditions to chronic pulmonary aspergillosis include:
Chronic Pulmonary aspergillosis usually presents with:
Answer to Q6
Allergic bronchopulmonary aspergillosis is a immunologic pulmonary disorder caused by a hypersensitivity to Aspergillus fumigatus. It presents clinically like chronic asthma (previously farmer’s lung disease). Steroids do not clear it completely, and, if left untreated, patients can develop bronchiectasis. It is therefore important to refer all asthma patients who do not improve on normal treatment for an Aspergillus IgE skin test.
Answer to Q7
Treatment depends on the clinical presentation. Aspergilloma is best treated surgically. Other forms might need embolization, surgery and antifungal agents.
The patient was prescribed itraconazole for a month after his surgery and has been very well ever since. He is on no other chronic medication for his pulmonary disease and will be followed up bi-annually.
In this case study we learned that many other conditions can mimic lung cancer. It is also important to not diagnose asthma or COPD too quickly. Treat lung infections correctly to prevent bronchiectasis and remember to look for aspergillosis in damaged lungs. If these conditions are not diagnosed and treated early they can cause irreversible lung damage.
References:
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®