
Dr John Black
A 39-year old lady presented to the Emergency department at the end of November 2013. She had a 3 week history of progressive dyspnea, non-productive cough and fever. In the 3 weeks prior to admission, she had been reviewed by her primary care facility and was found to be HIV-infected with a CD4 count of 143 cells/mm3. She was screened for TB with a Gene Xpert (GXP), which was negative, and treated with Amoxicillin. Her illness had progressed despite this, which prompted her presentation to hospital. Her past medical history was unremarkable, being employed as a domestic worker. She had never smoked, was not on any medication and had no significant exposure history.
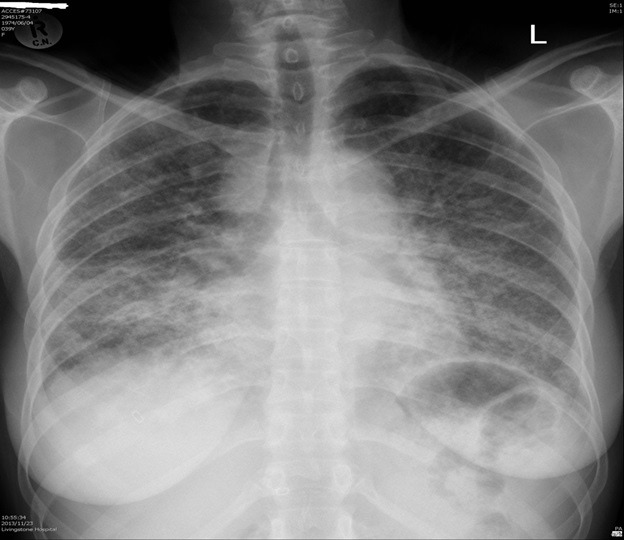
She was acutely ill, temperature 39°C, BP 135/85, Pulse 157 and oxygen saturation of 82% on room air. She had no palpable lymphadenopathy, oral or cutaneous lesions, but bilateral crepitations were noted on chest auscultation. Her WCC was 8.82 x 109/L, HB 12.6 g/dL and Plt 501 x 109/L. The CRP was 57 and the CEU was normal. A repeat GXP was negative.
Question 1: What is the differential diagnosis?
Answer to Q1
The three week history is unusual for a community acquired pneumonia with common viral or bacterial pathogens. The sub-acute presentation is more suggestive of tuberculosis (TB) or Pneumocystis jirovecii pneumonia. The clinical presentation and radiological features would favour Pneumocystis pneumonia (PCP), although there is a suggestion of lymphadenopathy in the right paratracheal region on CXR, which would be more compatible with TB.
Case Continued:
The patient was felt not to be a candidate for ICU and was treated for PCP with high dose co-trimoxazole and prednisone, and ceftriaxone for bacterial pneumonia. The original sputum TB culture was reported as negative. She improved over the following week and was discharged to the clinic on a tapering prednisone dose and co-trimoxazole with a view to starting antiretroviral therapy (ART). She stayed home for Christmas and only presented to the clinic in early January with worsening dyspnea and persistent cough. She was empirically started on TB treatment and continued her co-trimoxazole secondary prophylaxis. She presented again the Emergency Unit at the end of January having deteriorated despite 3 weeks of TB therapy. She had yet to start ART.
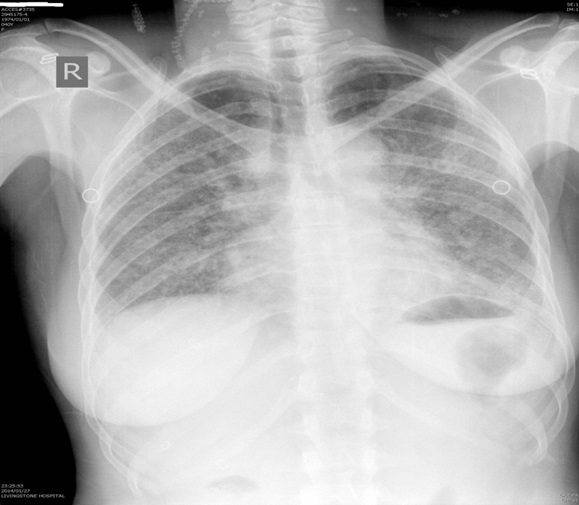
She was hypoxic, 87% O2 saturation on room air, apyrexial and had a BP of 114/80 and pulse of 133. Bilateral crepitations were again heard, but the examination was otherwise unremarkable. WCC 5.5 x 109/L, HB 16.2 g/dL, platelets 308 x 109/L and CRP 14. Her CEU and LFT’s were normal. A CXR was done:
Question 2: What are the possible causes for her readmission?
Answer to Q2
Recurrence of PCP is not an unusual phenomenon and is thought to occur in 3-4% of cases.1 In a study of 457 patients receiving secondary prophylaxis post PCP infection, there were no cases of recurrence over 363 person years follow up in those with a CD4 count >200 cells/mm3, including the 51 who stopped PCP prophylaxis. There was a total of 18 recurrent episodes and 6 out of 9 people who stopped prophylaxis with CD4 counts < 200 cells/mm3 had PCP recurrence. Recurrence was associated with low CD4 counts and stopping prophylaxis,2 but it has been described as part of an IRIS phenomenon.1
Sulfonamides act by interfering with folate synthesis through inhibiting dihydropteroate synthase (DHPS) which catalyzes the condensation of para-aminobenzoic acid and pteridine to form dihydropteroic acid.3 Pneumocystis jirovecii cannot be cultured, but it is postulated that reduced susceptibility to co-trimoxazole occurs through nonsynonymous point mutations, resulting in amino acid substitutions at positions 55, 57 or both in the DHPS region. Based on homology with the E. coli DHPS, these mutations appear in the active site of the enzyme involved in substrate binding that could result in structural changes which are thought to affect substrate binding and enzyme activity. Similar mutations are seen in Plasmodium falciparum and Mycobacterium leprae causing sulfa resistance.3 85/151 (56%) of samples from a SA study showed the same mutations in the DHPS region and highlighted the selective pressure high volumes of sulfa use have had on Pneumocystis.4
The clinical significance of these DHPS mutations must be inferred from correlating the clinical outcomes with the presence of DHPS gene mutations in patients with PCP. Clinical correlations of treatment failure have been contradictory, with some studies finding associations with mutations, whilst others correlate with specific Pneumocystis genotypes (type7) and some with clinical correlates, specifically with need for ventilation.5,6 Infection with Pneumocystis jirovecii type 6 was associated with prophylaxis failure and milder disease and is thought to be due to the propensity of the specific Pneumocystis strain to accumulate more mutations under selective pressure combined with spread of the strain in the community.7,8 Thus failure of treatment of acute episodes is likely a combination of severity factors, mutations and genotype. Failure of secondary prophylaxis is a combination of poor compliance, failure to immunologically reconstitute, possible resistance mutations and possible genotypes.
A clinical diagnosis of PCP recurrence was made and she was restarted on high dose co-trimoxazole, prednisone and continued her TB Rx. No respiratory sampling was performed. She made a steady recovery over 2 weeks and although she never recovered to her baseline, she was discharged having started ART (tenofovir/lamivudine/efavirenz) in hospital to continue her TB Rx, prednisone and co-trimoxazole prophylaxis at the clinic.
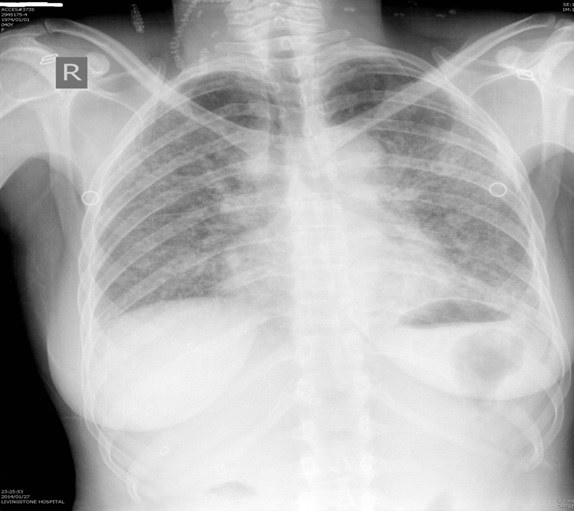
She subsequently was readmitted in April 2014 following a week history of dyspnea and a productive cough. She was afebrile, O2 saturation 78% and haemodynamically stable. WCC 7.5 x 109/L, Hb 14.3g/dL and platelets 506 x 109/L. Her CXR was done:
Question 3: What further tests would you do at this stage?
Answer to Q3
The history of recurrent admissions for respiratory failure despite treatment of the common respiratory pathogens should alert the clinician to the possibility of an underlying lung disease as mentioned in answer 2. In addition, PCP immune reconstitution inflammatory syndrome (IRIS) should also be considered. The possible tests include:
The patient was considered too unstable for a bronchoscopy or open lung biopsy. She was restarted on prednisone and a HRCT was done.
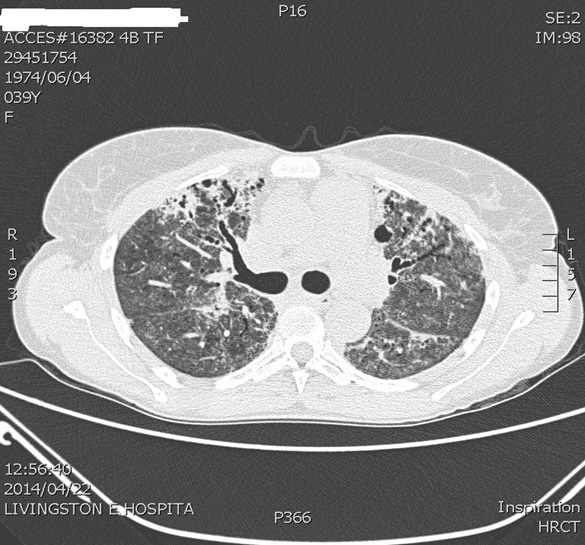
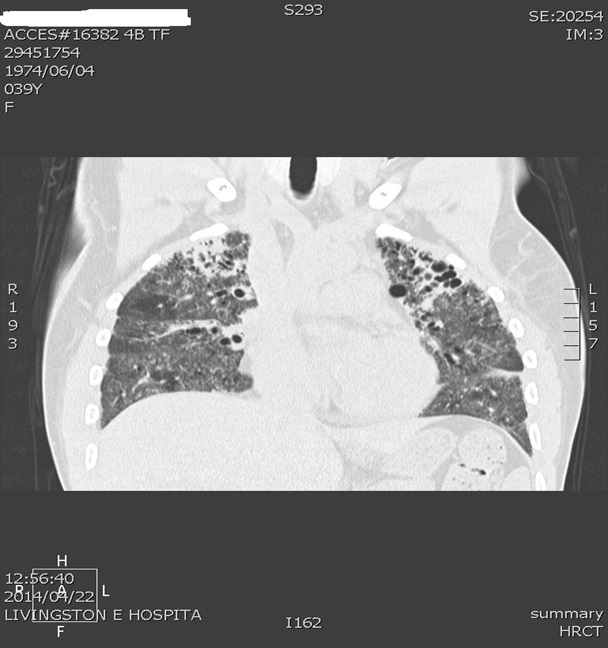
The HRCT showed diffuse ground glass opacification with bilateral asymmetric central bronchiectasis affecting predominantly the upper lobes, with bronchial wall thickening. Multiple pre- and para-tracheal lymph nodes were present, with sizes varying between 11-14mm. The features were suspicious of Non-specific Interstitial Pneumonitis. In the absence of an open lung biopsy, she was diagnosed with an HIV associated Interstitial Lung Disease, not specified based on the HRCT and there was some clinical improvement on steroid therapy. Her 6-week lung function tests showed a restrictive pattern with both the FEV1 and FVC at 28% predicted, with a ratio of 85% and the lung diffusion capacity was 35% of predicted. She remains on immune suppression with a limited effort tolerance.
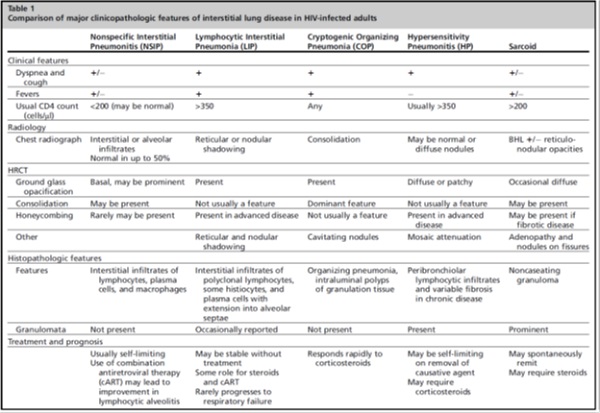
There are a wide variety of interstitial lung diseases associated with HIV (Table 1).9 Prior to the advent of ART, lymphocytic interstitial pneumonia (LIP) and non-specific interstitial pneumonitis (NSIP) were commonly described, whilst sarcoid is a disease seen in the ART era and may represent an immune reconstitution phenomenon. Drug induced hypersensitivity pneumonitis and cryptogenic organizing pneumonia are rare causes of pneumonitis described in HIV. Finally HIV seroconversion pneumonitis has been described as part of the primary HIV infection, which is a sub-acute pneumonitis that may mimic PCP.9
Non-specific Interstitial pneumonitis is part of a spectrum of lymphocytic pulmonary syndromes and is thought to be related to a cytotoxic T cell mediated response within the lung to structural HIV proteins. The clinical presentation can be similar to PCP, and in a series of 351 HIV-infected patients presenting with PCP like symptoms, NSIP was the most common diagnosis, seen in 15/67 PCP negative cases.10 Dyspnoea, fever and cough are the most common features and the fever may be prolonged. The CD4 count is usually < 200 cells />mm3 and the degree of hypoxia is variable. Radiologically there are 3 patterns on CXR, with 50% demonstrating a normal radiograph, and the remainder either interstitial infiltrates or alveolar infiltrates. Effusions and lymphadenopathy are unusual. HRCT has no pathognomonic features, but features described include predominantly basal ground glass infiltrates, areas of consolidation and rarely honeycombing.
NSIP is usually self-limiting and can remain stable for years or regress spontaneously. Rarely steroids are indicated and the lymphocytic alveolitis may also regress on ART itself.9
Lymphocytic Interstitial pneumonia (LIP) usually occurs in HIV-infected children and is uncommonly described in HIV-infected adults and can occur as part of a Diffuse Infiltrative Lymphocytosis Syndrome (DILS). Constitutional symptoms are a prominent feature, exertional dyspnea and a non-productive cough occur in the majority of patients. Clinical features of DILS may also be found, which include lymphadenopathy, hepatosplenomegaly, parotidomegaly, multiple neurological manifestations and associated xerophthalmia and xerostomia. The CD4 count is usually maintained and variable degrees of hypoxia occur. In an unpublished series from Groote Schuur Hospital over 6 years (Naidoo et al), 13 biopsy-proven cases were identified. The majority of patients were young females with a median CD4 count of 194 and symptom duration of 5 months who were referred for non-resolving TB. 50% had lymphadenopathy on CXR and none exhibited clubbing of the fingers.
Radiologically there are 3 main patterns on CXR, which include fine basal reticulonodular opacities, a miliary like pattern with larger nodular opacities and reticular infiltrates and a dense alveolar infiltration with micronodules and reticular shadowing. HRCT demonstrates reticular shadowing, centrilobular nodules and areas of ground glass opacification with interstitial infiltrates. Fibrosis and honeycombing may be visible and when there is associated DILS, lymphadenopathy may be evident. The most common infective differential diagnosis still remains PCP, however mycobacterial diseases need to be considered as well. The diagnosis is confirmed on biopsy and the exclusion of other opportunistic infections.
LIP rarely progresses to respiratory failure and death, and the disease can be stable for months without specific treatment. Steroids are used in the treatment of LIP, with variable lengths of treatment, and more aggressive immune suppression may be used with co-existing DILS. LIP-IRIS has also been described.9
PCP remains a clinical diagnosis in many cases. Bronchoscopy with BAL and molecular diagnostics are not readily available in many centres and clinicians treat based on the clinical picture. Selective pressure from programmatic co-trimoxazole use has caused widespread mutations in key genes that may affect co-trimoxazole susceptibility, but the clinical significance of this is uncertain at this stage. PCP recurrence does occur, but usually occurs at low CD4 counts in the absence of co-trimoxazole prophylaxis.
Whilst ILD in HIV is an uncommon disease, it shares many features with common opportunistic infections. In patients who present with atypical or refractory/relapsing opportunistic infections where no infective agent is found, ILD needs to be considered in the differential diagnosis. They generally follow a benign course, however, as with our patient, some progress to respiratory failure requiring long term immune suppression.
References:
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®