
Rispah Chomba and Warren Lowman
Male, 38 yrs old, previous pulmonary TB in 2009 treated for 6 months. HIV diagnosed in Aug 2010 when he presented to the surgeons with a chest mass and draining sinus. He was treated with 9 months of TB therapy despite negative cultures, and started on ART (TDF, 3TC, EFV).
In March 2011 he was re-admitted with cough, chest pain radiating to the back and right cervical lymphadenopathy. A fine needle aspirate of the nodes was performed.
Aspirate MC&S grew a Nocardia spp identified on 16SrRNA sequence analysis as N. brasiliensis
MIC testing (by broth microdilution [BMD]) showed the following susceptibility:
The patient was allergic to TMP-SMX and was treated for 5 weeks with amikacin and ceftriaxone (the reasoning behind the choice is unknown), and discharged home on amoxicillin-clavulanate 625mg TDS.
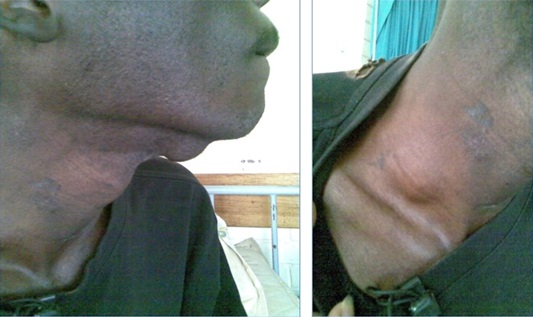
Three months later, his outpatient notes state that the sinus on chest wall now closed but patient has a central neck mass. Goitre? Cyst? Patient noticed increasing size over last 6 days. Patient referred to the surgeons. Ultrasound revealed a complex cystiEDc mass in the left lobe of thyroid most likely infective. Over the next week the anterior neck swelling enlarged with associated dysphagia and dyspnea.
On examination, he was wasted, afebrile, with a tender, enlarged goitre and generalized shotty lymphadenopathy. Investigations showed:
On the advice of the endocrinologists, prednisone and Luggol’s iodine was started. An ultrasound-guided aspiration of thyroid mass aspirated 18ml of pus from the left lobe followed by incision and drainage. Definitive surgery was not performed due to the risk of thyroid storm. Steroids were stopped after 10 days.
Four days after the I&D, the patient complained of diarrhoea and stool was positive for C. difficile toxin. Treated with metronidazole.
Pus cultured from thyroid aspirate grew N. brasiliensis
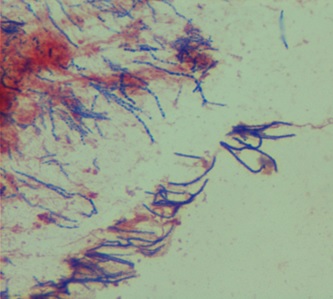
Modified Kinyoun stain of thyroid biopsy
The patient developed a right supraclavicular swelling which was incised & drained.
On the basis of his new resistance profile, he stopped amoxicillin-clavulanate and started linezolid 600mg BD.
A CT brain confirmed a poorly enhancing multi-cystic right cerebellar hemisphere mass with surrounding oedema, early hydrocephalus and attenuation of 4th ventricle. Large necrotic submental nodes and multiple necrotic mediastinal and anterior neck nodes were noted on lower cuts.
Laboratory Diagnosis of Nocardia Species
Diagnosis of nocardiosis can be challenging as the organism is relatively slow-growing and often overgrown by other micro-organisms. The first clue to the presence of a Nocardia species is the Gram stain, which typically demonstrates filamentous beaded Gram positive bacilli. A modified Kinyoun stain that then demonstrates acid-fast bacilli is further supportive evidence and attempts should be made to isolate this organism through use of selective media.
Upon isolation of what appears to be a Nocardia species (typical chalky-white, cotton-wool appearance, musty smelling colony) a definitive genus and species identification can only be made using molecular diagnostic modalities. Biochemical tests e.g. hydrolysis reactions are generally indiscriminatory and unreliable.
Commercial identification systems have similar limitations to traditional phenotypic methods and are unreliable. Despite its widespread use and applicability in bacterial identification MALDI-TOF has not demonstrated sufficient accuracy in the identification of aerobic actinomycetes, including Nocardia spp. This is possibly related to the lack of a suitably representative database.
Serological tests play no role in the diagnosis of nocardiosis. Molecular methods including 16S rRNA and other target gene (e.g. secA, HSP-65) sequencing are currently the gold standard for species ID, although there are limitations in interpretation of sequence data.
Antimicrobial Susceptibility Testing of Nocardia
Norcadia Thyroiditis
Thyroiditis due to nocardia is a rare presentation and there are only four cases reported in the literature:
It is important to note that these cases present N. asteroides as the causative species. This is probably inaccurate and these are considered cases of misidentification. N. asteroides was the name assigned to the reference strain ATCC 19247, but this was prior to molecular testing and given the inert biochemical nature of nocardia isolates many different species appear biochemically the same. Clinical strains of nocardia have not been found to match the original type strain (according to sequence-type). The taxonomic nomenclature of nocardia remains in a state of flux but the species name N. asteroides should no longer be used to designate the most commonly identified cause of nocardiosis. In all likelihood this species name will be confined to the microbiological history books. Interestingly isolates defined as N. asteroides are typically found to be identical to N. cyriacigeorgica.
References:
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®