
Helena Rabie, Rabeen Lutchman and Mark Cotton Tygerberg Hospital
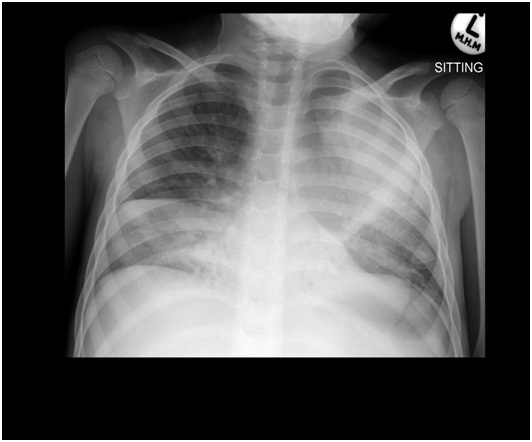
A 6-year-old HIV infected boy who previously defaulted antiretroviral therapy, presented with a chronic cough that worsened in the prior 4 weeks. He also complained of increasing shortness of breath and fever for the past 3 weeks.
He had presented to his local clinic in the 3 months prior to admission, and been diagnosed with pulmonary tuberculosis based on symptoms and a suggestive chest radiograph. Sputum smear was negative and culture not requested. At this time his HIV viral load was log 4.64 copies/ml and the CD4 count 2 cells/mm3.
Therapy with rifampicin, isoniazid, pyrazinamide, abacavir, lamivudine, and efavirenz was started at the local clinic.
His mother regularly attended tuberculosis and antiretroviral clinic and on interview, a good understanding of medication routine was noted.
Examination revealed a chronically ill-looking boy with acute, severe respiratory distress requiring supplemental oxygen
His HIV viral load on admission had suppressed and his CD4 count had increased to 210 cells/mm3. Sputum smear was positive for acid fast bacilli.
Question 1: What is the differential diagnosis?
Answer to Q1
The differential diagnosis this child should include the following:
Question 2: Which test/s would you request next?
Answer to Q2
Line probe assay or Xpert® MTB/RIF should be requested to try and rapidly asses for drug resistant tuberculosis
Sputum for Xpert® MTB/RIF was requested twice and was found to be negative on both occasions.
Question 3: How does this result influence you thinking?
Answer to Q3
This suggests that the patient does not have tuberculosis. In the case of this child Mycobacterium avium-intracellulare infection was confirmed on numerous sputum cultures. In our case we did not confirm dissemination as the blood culture was negative and bone marrow aspiration and culture was not done. The abdominal ultrasound was normal.
Non-tuberculous mycobacteria (NTM) are widespread in the environment including water, soil, food products and domestic and wild animals. More than 130 species, not all human pathogens, have been identified. The organisms cause a variety of infections and presentation will depend on the species and the host. Table 1 represents a classification of NTM according to growth pattern.
Table 1: Classification of nontuberculous mycobacteria*
| Rapidly growing nontuberculous mycobacteria |
| M. fortuitum complex |
| M. fortuitum |
| M. peregrinum |
| M. porcinum |
| M. chelonae |
| M. abscessus |
| M. abscessus |
| M. bolletii (previously M. massiliense) |
| M. smegmatis |
| M. mucogenicum |
| Slowly growing nontuberculous mycobacteria |
| Photochromogens |
| M. kansasii |
| M. marinum |
| Scotochromogens |
| M. gordonae |
| M. scrofulaceum |
| Nonchromogens |
| M. avium complex |
| M. avium |
| M. intracellulare |
| M. terrae complex |
| M. ulcerans |
| M. xenopi |
| M. simiae |
| M. malmoense |
| M. szulgai |
| M. asiaticum |
| M. haemophilum |
Rogall T, Wolters J, Flohr T, Böttger EC (October 1990). "Towards a phylogeny and definition of species at the molecular level within the genus Mycobacterium". International journal of systematic bacteriology 40 (4): 323–30.
Runyon EH (January 1959). "Anonymous mycobacteria in pulmonary disease". The Medical clinics of North America 43 (1): 273–90.
Brown-Elliott BA, Wallace RJ (October 2002). "Clinical and taxonomic status of pathogenic nonpigmented or late-pigmenting rapidly growing mycobacteria". Clin. Microbiol. Rev. 15 (4): 716–46.
There are well-described clinical syndromes of NTB in children (table 2).. In addition some organisms are specific to geographic areas.
Epidemiology
There is increasing recognition of pulmonary NTM infection in children in the context of underlying lung disease. In addition geographic factors may influence risk
Clinical features of pulmonary disease:
In the literature clinically significant NTM pulmonary disease is most often described in children with preexisting lung disease (eg, cystic fibrosis).The features depend, to some extent, upon the underlying medical condition. Symptoms and signs include:
The species may influence the findings
If NTM is suspected it is advisable to contact the laboratory personnel at the time specimens are taken to ensure that optimal growth.
Sputum smear positivity is variable. Traditionally organisms take 2-4 weeks to grow on solid media and 1-2 weeks in liquid methods.
Commercial DNA probes and 16S rRNA gene sequencing can facilitate more rapid diagnosis and speciation. The GeneXpert system permits rapid detection of M. tuberculosis complex and rifampin resistance, but has not been developed for NTM.
Susceptibility or resistance does not always correlate well with clinical efficacy. The exception is of clarithromycin resistance for treatment of disseminated or pulmonary MAC, clarithromycin resistance for M. chelonae and M. abscessus infections, and rifampin resistance for pulmonary M. kansasii.
Diagnostic criteria for pulmonary disease.
The diagnostic criteria for pulmonary disease as per the American Thoracic Society are noted below, however there is no validation in children.
Therapy
The isolation of NTM from respiratory specimens does not necessarily suggest that therapy is needed. The clinical relevance should be determined and therapy only instituted if it is thought to be relevant.
M. avium complex (MAC)
Therapy of HIV uninfected children should take into consideration the extent of disease:
Nodular or non-cavitating bronchiectatic MAC lung disease should be treated with a regimen that includes
Extensive bronchiectasis or fibrocavitary MAC lung disease is treated with
The macrolide, ethambutol, rifamycin and aminoglycoside should be administered daily in children but in older adolecents the aminoglycoside can be given 3 times per week. The aminoglycoside should be discontinued after eight weeks;
HIV-positive children who meet the diagnostic criteria for pulmonary disease should be treated in the same manner as those with disseminated infection.
Children should be treated until the sputum is negative for 12 months.
The aminoglocoside can be discontinued after 2 months of improvement is shown.
M. abscessus
M. abscessus has a predilection for infecting diseased lungs and is difficult to eradicate; cure is possible only with surgical resection when lung disease is limited The goal of M. abscessus therapy is not eradication but rather symptomatic and radiographic improvements. Therapy should include three drugs to which there is documented susceptibility; after four to eight weeks of intensification therapy, two drugs may be used to complete therapy (usually 6-12 months). The regimen often includes:
There have been no randomized trials of treatment for M. kansasii
Treatment should continue until sputum cultures have been negative for at least one year.
Rifampin-resistant isolates should be treated with three drugs based upon in vitro susceptibilities. Potential agents include macrolides, fluoroquinolones, aminoglycosides, and trimethoprim-sulfamethoxazole.
This case illustrates a number of important points with regards mycobacterial diagnosis
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®