
Dr John Black, Division of Infectious Diseases and HIV Medicine, UCT
A 38 year old man from the Eastern Cape presented to a Cape Town hospital with acute diarrhoea. He had been diagnosed with HIV in 2009 (CD4 count of 1 cell/mm3) and was initiated on first line ART. He subsequently failed first line therapy and was switched to Tenofovir, Lamivudine and Aluvia in 2012 when his CD4 count was 55 cells/mm3.
He was markedly wasted (38kg), with diffuse impetigo and multiple subcutaneous abscesses. MRSA was cultured from pus draining from one abscess, as well as a non-typhi Salmonella from stool.
His abscesses was drained and treated with Vancomycin for 4 days followed by topical Mupirocin. His skin cleared rapidly and his diarrhoea settled without treatment.
He subsequently developed an unexplained neutropenia, with a WCC 1.7 x 109/L (absolute neutrophil count 0.13 x 109/L). Three days later, he developed new skin lesions (see figures) and a high spiking fever. Blood cultures were taken and he was started back on Vancomycin to cover what was thought to be a recurrence of the staphylococcal skin lesions.
A Gram-negative bacillus was subsequently cultured from blood cultures sets and a pus swab from one of the new skin lesions.
Question 1: What is the likely clinical diagnosis of the skin lesions?
Answer to Q1
Ecthyma gangrenosum (EG).
There are 2 major routes for the development of EG.
Haematogenous dissemination of the bacteria or fungus to skin Primary cutaneous EG - a non-bacteraemic form in which the skin lesions are located at the site of inoculation.
Preferred sites are the axillary and perianal regions, although any region may be affected. On average, 50% of lesions are located in the gluteal and perineal regions, 30% on the extremities, and 12% on the face and body.10 Occasionally, EG may appear as a local complication of a wound infected with the microorganism and although blood cultures are initially negative, secondary bacteraemia and clinical decompensation may occur if treatment is delayed.1,9 Primary cutaneous EG generally has a better prognosis, than the classic bacteraemic (fungaemic) form.
Clinically, EG starts as an inflammatory plaque, papule, or macule, reddish in colour, oedematous, and painful, which in less than 12–24 h develops into a haemorrhagic blister, vesicle, pustule or nodule with a narrow inflammatory rim. After the blister bursts, there remains a non-odorous central necrotic ulcer covered by a blackish scab surrounded by a light coloured zone and an elevated purplish erythematous external ring which is infiltrated to the touch.1,10 In primary cutaneous EG, there are normally few lesions; however, in EG that is associated with sepsis, there are usually multiple lesions. EG in children has the same clinical characteristics as in adults.1
Histologically EG is characterised by 3 features.10 Bacterial invasion of the media and adventitia of the vein walls in the dermis, with sparing of the intima and lumen. The absence of inflammation is a marked feature.
Bacterial invasion results in marked fibrin exudation and haemorrhage, followed by bullae formation Necrosis of the dermis is the final stage
Bacteria are readily visible on Gram stain of biopsy samples and from material scraped from the base of the lesion.1,10
Question 2: What organism is classically associated with this condition?
Answer to Q2
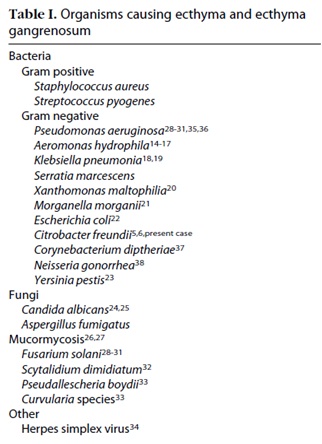
This is the classic cutaneous lesion associated with Pseudomonas infection. However, cases have been described of lesions similar to EG produced by other organisms (Table 1)2
Pseudomonas. Aeruginosa (P. aeruginosa) is a Gram-negative bacillus that is a component of the normal intestinal flora. Although it cannot survive on intact, dry skin, P. aeruginosa can colonise moist intertriginous areas, such as the groin and axillae which explains the frequent localization of P. aeruginosa EG to these areas1. The vascular destruction that leads to EG lesions in septicaemia due to P. aeruginosa is thought to be related to dissolution of the elastic lamina by pseudomonal elastase1,9. Not unexpectedly, other bacteria (e.g. Aeromonas maltophilia)2,3 that have been implicated in the development of EG also produce elastase and various proteases.2,9 Likewise, several of the opportunistic mycoses that can cause lesions resembling EG (e.g., aspergillosis, fusariosis, zygomycosis) have a propensity to invade blood vessel walls, resulting in thrombosis and tissue necrosis.
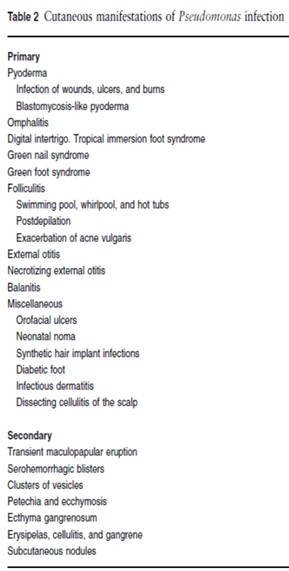
Pseudomonas sepsis occurs mainly in immunocompromised patients. Additional risk factors include advanced age, receipt of antimicrobial therapy within past 30 days, and presence of a central venous catheter or a urinary device.4 The most common primary foci are the respiratory system, gastrointestinal and genitourinary tracts, skin, and soft tissue. Clinically, it is indistinguishable from sepsis produced by other bacteria, except for the presence of associated skin manifestations.1,10 Cutaneous manifestations may occur in 1.3-13% of cases of Pseudomonas sepsis1 (between 20 and 50% in children)9 and the range of skin lesions associated with P. aeruginosa sepsis includes: vesicles and bullae, subcutaneous nodules, gangrenous cellulitis, ecthyma gangrenosum and maculopapular lesions.1,10 The development of these lesions in a patient with risk factors should strongly suggest the presence of Pseudomanas bacteraemia and presumptive antimicrobial management should cover this organism as the mortality associated with a delay in appropriate antimicrobial cover for Pseudomonas sepsis may exceed 40%.5,10
The full range of skin infections due to Pseudomonas is shown in table 2.1
Question 3: What are the predisposing factors for this condition?
Answer to Q3
Predisposing factors
Abnormal neutrophil function (resulting from quantitative or qualitative defects) represents the most important risk factor for both disseminated P. aeruginosa infection and opportunistic mycoses1. Almost half of paediatric patients with EG have leukemia or aplastic anaemia, and the occurrence of EG usually coincides with neutropenia related to the administration of chemotherapy or myeloablative regimens for peripheral blood stem cell transplantation.
Additional predisposing factors for the development of EG in cancer patients and other immunocompromised hosts include prior antibiotic therapy, treatment with systemic corticosteroids or other immunosuppressive medications, diabetes mellitus, hypocomplementaemia, occlusion or maceration of the skin, and, particularly in premature neonates, a high-humidity environment.1,9,10 Pseudomonas sepsis is not a common infection in HIV, with only 1/3 being ascribed to neutropenia, however EG has been described in both neutropenic and non-neutropenic patients and may be associated with a high recurrence rate.6,7
Intravenous catheters and invasive procedures represent additional iatrogenic risk factors. Finally, bacterial contamination (e.g., with P. aeruginosa) of “moist” hospital equipment and supplies, ranging from nebulizers to antiseptic solutions, can be a source of nosocomial infections manifesting as EG in immunocompromised patients9.
Approximately one third of reported paediatric cases of EG occurred in previously healthy children. The median age of these patients was younger than 1 year, compared with approximately 4 years for children known to have an underlying medical disorder. Most cases developed in the setting of an acute gastrointestinal illness, and more than half the children were subsequently found to have X-linked recessive agammaglobulinemia or another immunodeficiency syndrome9.
Cutaneous lesions that may be clinically identical to pseudomonal EG can also be seen in the setting of disseminated fungal infections: candidiasis (10% to 15% of cases), aspergillosis (< 5% of cases) and fusarium (70% to 90% of disseminated infections) should also be considered as part of the differential diagnosis.9
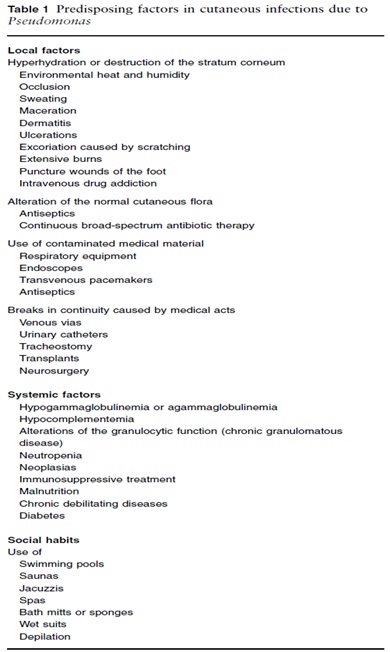
A list of predisposing characteristics is shown in table 31
References
The patient cultured Pseudomonas aeruginosa from both his blood cultures and from a pus swab taken from the base of the necrotic lesions. His Vancomycin was stopped and he received high dose Ciprofloxacin 750mg bd, as directed by antimicrobial susceptibility testing, with a good clinical response. His neutropenia resolved with the treatment of his sepsis and he was discharged home after a prolonged hospital stay.
A delay in appropriate antibiotic therapy is associated with a high mortality in Pseudomonal sepsis. A clinical diagnosis of Ecthyma Gangrenosum should prompt the initiation of antimicrobials with Pseudomonal cover.
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.

Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®