
J Klotnick, SASTM
A 63-year old woman presented with intermittent fevers and rigors three weeks following her return from a one month trip to South East Asia. While away, she had a short episode of diarrhoea with no sequelae. No rash, cough, shortness of breath or urinary symptoms were reported. She had no contact with animals and does not recall any insect bites.
Question 1: What important information is required prior to embarking on an examination and further investigation?
Answer to Q1
1. Past and current medical history
She has rheumatoid arthritis (RA). She was on maintenance therapy of methotrexate and plasmoquine for more than twenty years. This was discontinued a year ago as she could no longer tolerate it and developed visual abnormalities from the plasmoquine.
She has no cardiac or respiratory disease history, and was on hormone replacement therapy for eight years. She stopped smoking when she was 35 years old.
gynaecological examination a year ago was normal.Vaccination history
Malaria chemoprophylaxis
Mefloquine, which she took one week prior to her trip, weekly whilst in SE Asia and for two weeks after returning to South Africa.
Detailed itinerary and accommodation
Her visit was to Vietnam, Cambodia and Singapore. She stayed in good accommodation and did not ‘eat off the street.’
Miscellaneous
Immersion in inland waterways, sexual exposures for HIV seroconversion, visits to live poultry markets
Question 2: What additional vaccinations should be considered for this traveller?
Answer to Q2
NB: Live vaccines are not contraindicated in this traveller as a year had elapsed since taking the methotrexate.
Question 3: With reference to non drug-related malaria prevention, what advice should be given to the patient prior to her travel to SE Asia or any malaria area?
Answer to Q3
Question 4: With reference to malaria
Answer to Q4
1. Plasmodium falciparum and Plasmodium vivax (Plasmodium malariae is rare)
2. Doxycycline 100mg, given 1 day prior to entering the malaria area, 1 tablet taken daily in whilst in the malaria area and for 28 days after leaving the malaria area. Take with plenty of fluid and after food. Doxycylcine may cause photosensitivity in around 3% of users and if not taken with food and fluid, may cause oesophageal ulceration
Mefloquine - To be taken one week prior to entering the malaria area, once weekly, whilst in the malaria area and weekly for FOUR weeks after returning from the malaria area. Adult dose is 250mg, and paediatric dose is weight-dependent; 5-19kg 62.5mg, 20-30kg 125mg, 31-45kg 187.5mg and >45kg, full dose. Tablets should be swalled whole after a meal with plety of fluid. If there is a concern about potential side effects, the medication should be started two weeks prior to entering the malarious area. Side-effects, including vivid dreams, anziety attacks, dizzyness and vertigo and gastrointestinal symptoms are the more common, and are generally encountered after the second dose. If these do occur, there is still time to switch to a different regimen.
Atorvaquone/proguanil - taken one day before entering the malaria area, once daily while in the malaria area and then once daily for seven days after leaving the malaria area. Adult dose and for children >40kg is 250mg/100mg and should be taken after food. Paediatric doses; 11-20kg 62.5/25 mg (1 paediatric tablet), 21-30kg 125/50 mg (2 paediatric tablets), 31-40kg 187.5/75 mg (3 paediatric tablets).
Question 5: What would be the more common causes of fever and rigors in this patient?
Answer to Q5
Clinical examination revealed hepatosplenomegaly and fever of 38.5oC. An abdominal ultrasound confirmed hepatosplenomegaly and a few enlarged non-specific lymph glands.
Question 6: What are the more common causes of fever and hepatosplenomegaly?
Answer to Q6
Blood tests on day 1 revealed the following:
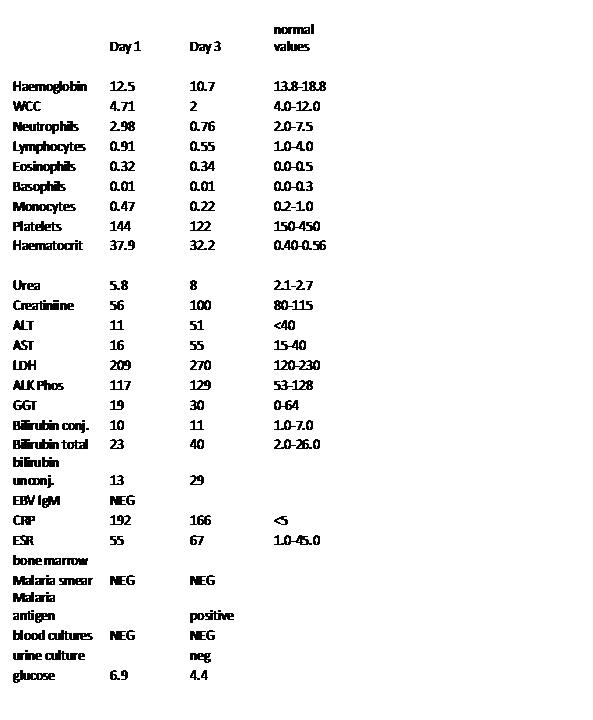
Question 7: What is your differential diagnosis in light of the blood results from day 1?
Answer to Q7
A bone marrow aspirate and biopsy showed a non-specific reactive bone marrow. Immunophenotypic analysis did not show any B cell lymphoproliferative disorder.
After 48 hours it was decided to repeat some of the blood tests and the malaria thin and thick films were negative, however the Plasmodium falciparum and common Plasmodium antigen were positive (See table day 3).
Question 8: What is the most likely diagnosis now?
Answer to Q8
In view of the drop in the blood counts and the positive antigen tests, without the documentation of parasites on the smear, it was decided with the help of a physician and a microbiologist to treat this patient empirically for malaria.
The treatment regimen selected for the patient was: quinine 600mg orally 8 hourly and Doxycycline 100mg daily. Her urine cultures and other blood cultures were clear.
Question 9: Which other conditions cause thrombocytopenia in a returning traveller?
Answer to Q9
Symptoms settled and the patient was discharged home.
However, a week after completing the malaria treatment fever without rigors returned, associated with fatigue and mild arthralgia. There were no cardiac or respiratory symptoms and no weight loss had occurred since her discharge from hospital. Low grade fever and hepatosplenomegaly were present. Repeat ultrasound showed the persisting abdominal lymph nodes and multiple para-aortic and inguinal lymph nodes.
Question 10: What would be the next most appropriate investigation?
Answer to Q10
Lymph node biopsy
Lymph node histology reported Hodgkin’s lymphoma. The patient was referred to an oncologist.
Any traveller that has been close to or entered a malaria area, whether the risk of getting malaria is high or not, a high index of suspicion for the disease must always be maintained despite an initial result or a subsequent malaria result being negative. A single malaria test does not rule out malaria. The clinician in the above case correctly repeated the blood tests despite the first test being negative. There are different reagents that are used in malaria test kits. A raised rheumatoid factor is known to cause a false positive malaria result. Did this lady truly have malaria or was this the underlying lymphoma or did she have both? We could not have left this lady untreated for malaria and assume that her symptoms were attributable to the lymphoma. The rapid deterioration in her biochemical markers, the positive malaria test (even if it was a false positive test), the unwell patient and the potentially fatal disease of malaria creates a fear in the treating physician that malaria is not to be ignored and should never be ignored. In a symptomatic or unwell patient, the risk of treating a positive malaria result, even if it be a false positive result, far outweighs the consequence of not treating the disease. In the above case, even if the result was a false positive result, treating the patient for malaria will have made no difference on the outcome of the lymphoma.
Another lesson learned from the above case is that communication with a patient/traveller is of utmost importance. What was the reason for the patient not completing her malaria chemoprophylaxis? Was it poor communication from the doctor at the initial travel consultation or was it the patient who defaulted treatment? The correct maintenance of malaria chemoprophylaxis needs to be stressed to all travellers. If for any reason a traveller does not complete the correct malaria chemoprophylaxis, a doctor, nurse, pharmacist, spouse, family member or even a friend, should be informed of this, as should the travellers’ condition deteriorate at any stage after travel or during travel, this information may be life saving to the traveller.
Thus, in summary: good communication, prevention of mosquito bites, use of chemoprophylaxis and a high index of suspicion of malaria in the returning traveller, enabling rapid diagnosis and treatment of the infection will reduce morbidity and mortality of malaria.
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®