
Dr Lisa Frigati, Dr Helene Rabie, Prof Mark Cotton, Tygerberg Hospital
A 6-year old girl presented to Tygerberg Hospital EU with a 4-month history of headache, dizziness and intermittent vomiting. She had been living in the Eastern Cape and travelled to Cape Town the day before. She was HIV-exposed but tested ELISA-negative at eighteen months of age, had no known TB contact, and had received her full course of immunization. She had normal development and no history of trauma.
Her head circumference was 55.5cm (>98th centile), but the shape was asymmetric with a ‘bony swelling’ over the right temporal area. She had mild facial asymmetry, a Glasgow Coma Score of 14/15, decreased power (4/5) in left upper and lower limbs, and a hemiplegic gait. The rest of her examination was normal.
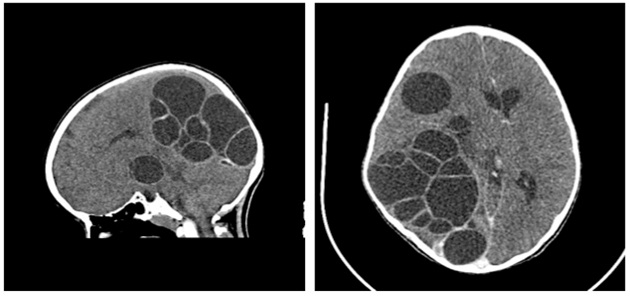
Full blood count and white blood cell differential was normal apart from thrombocytosis 556 X109/L. An urgent CT scan was requested:
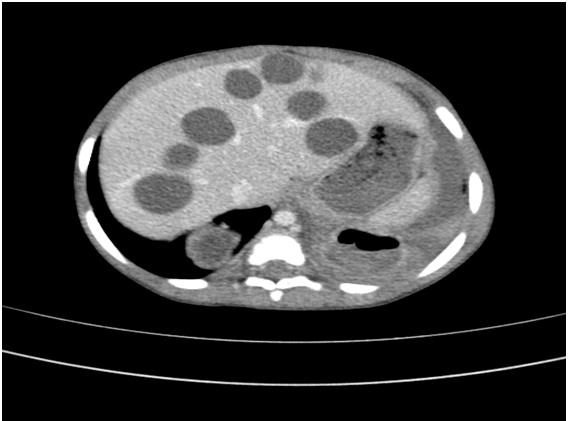
Abdominal utrasound showed 7 simple liver cysts in the left and right lobes, the largest measuring 4.2 x 4cm.
Chest X-ray was normal.
Question 1: What is the diagnosis and describe the life cycle of the organism?
Answer to Q1
1. Diagnosis and life cycle of the organism
This child has cystic echinococcosis or hydatid disease, which is multifocal with multiple intracranial and hepatic cysts.
Cystic echinococcosis is a zoonosis caused by cestodes (tapeworm) of the Echinococcus granulosus complex. In contrast, alveolar echinococcosis is caused by Echinococcus multilocularis, whereas polycystic or ‘neotropical’ echinococcosis is cause by Echinococcus vogeli or Echinococcus oligarthus both of which are confined to Central or South America (1).
E granulosus species comprises several different taxa, which influence adult morphology, host preference and human and animal pathogenicity. Ten strains have been described (G1-10) however some of these strains have been re-classified as separate species on the basis of molecular differences (2). E granulosus (G1-3) is believed to cause most human cases.
E felidis (‘lion strain’) is the only strain not using the domestic dog as a host (3). E equinis (G4) is considered the only species that cannot infect humans.
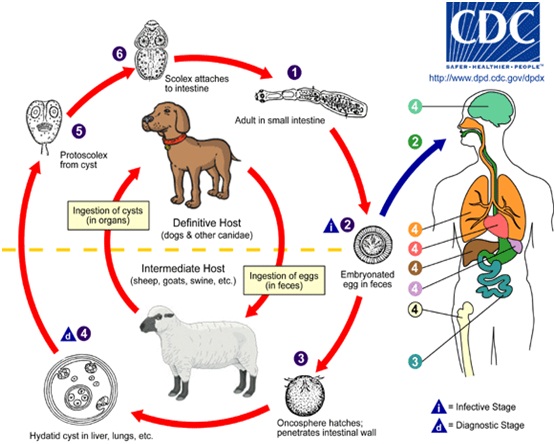
The dog is the usual definitive host, housing the reproductive phase of echinococcus. Sheep are the main intermediate hosts and ingest ova. Which form cysts, later consumed by the dog (See below).
Humans accidentally acquire echinococcosis by ingesting viable eggs shed in faeces of tapeworm-infected canines. Ova are resistant to desiccation, remaining viable for many weeks and can be transmitted to people without direct contact to the intermediate host. In the human gastrointestinal tract the ova hatch to form onchospheres that penetrate the mucosa, enter the circulation and encyst in host organs, developing into mature larval cysts.
Infection is usually acquired during childhood and manifests with symptoms in adulthood. The higher prevalence among rural/semi-rural children in South Africa may relate to farming and domestic activities and because of the close contact between children and dogs (4). Dogs should not be allowed to feed on carcasses of infected sheep and stray dog populations should be controlled. Teaching children regular hand washing will also help.
The brain is the site of cyst formation in 1-2% of all echinococcus infections (5,6) with 50-75% of cases occurring in children (7). Approximately 30 cases of primary and secondary multiple hydatid cysts in the brain have been reported (5,6). Compressible organs facilitate growth of the cyst and it has been proposed as a reason for the apparent prevalence of lung and brain involvement in children (8). Cysts are usually large, solitary, with minimal inflammatory response. Headache and vomiting are the most common presenting complaints. Seizures are rare. Clinical signs depend on the size and location of the cysts with the most common being hemiparesis, visual deficit and diplopia (9).
Question 2: What diagnostic tests should be performed?
Answer to Q2
2. Diagnostic tests for human echinococcosis
Echinococcus granulosus enzyme immunoassay (EIA) was the test used to diagnose this patent. It was positive with a ratio of 10.2 (Reference range: < 0.9: negative; 0.9 -1.1: equivocal; > 1.1: positive). Sensitivity of serology depends on the site of the cysts; 90% in liver and lung cysts, but less sensitive for other organs (1). New assays are being developed using recombinant echinoccocal antigens. Eosinophilia may or may not be present.
Imaging (ultrasound, CT and MRI) is more sensitive (90%) than serodiagnostic techniques (1) and a suggestive scan with negative serology is highly suggestive of echinococcosis.
Intracranial hydatid cysts are typically decribed on CT as large, round, well-defined, thin-walled, homogeneous, low-density cystic lesions without surrounding oedema and enhancement (9,10).
On MRI, cysts have a signal density similar to CSF and a rim of low signal on T1 and T2 weighting. MRI may also show peri-lesional oedema not seen on CT and is the preferred investigation for intracranial cysts (10). A retrospective review over 3 years from a South African tertiary hospital reported 21 cases, 8 of which had multifocal disease. Extended imaging is recommended to identify multifocal disease, which may also display complicated cysts, e.g. those that communicate with the biliary tree or those that are infected (10).
Question 3: How would you manage this child?
Answer to Q3
3. Management of intracranial hydatid cysts
Treatment of intracranial hydatid is surgical. Dowling’s technique is used to remove the entire cyst(s). Albendazole is given before and after surgery to minimize the risk of spread if there is spillage intra-operatively. Steroids are not usually indicated as there is minimal oedema surrounding the cysts. Albendazole 15mg/kg for 28 days is the drug of choice in children, superior to Mebendazole because of greater GIT absorption leading to higher plasma levels. The overall response rate to albendazole in adults and children is 55-79%, with cure in 29% of cases (1). However, a recent review has questioned albendazole’s efficacy (12). Praziquantel and Nitazoxanide have some activity against cystic echinococcosis (13-15).
Question 4: At which other sites might you may find these cysts?
Answer to Q4
4. Other sites of hydatid disease in children
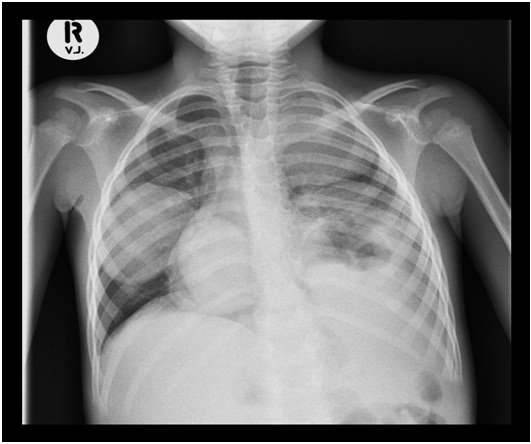
The most frequent site of involvement is the lung (11).
Unusual sites include:
The lung in children is more elastic and therefore more compressible (8). In these sites, cysts enlarge more rapidly and cause symptoms earlier resulting in early detection.
The following exemplify some of the pediatric cases seen at Tygerberg Children’s Hospital (courtesy of Dr. Pierre Goussard).
Pulmonary Hydatid Cysts on CXR
Liver Hydatid Cysts on CT scan
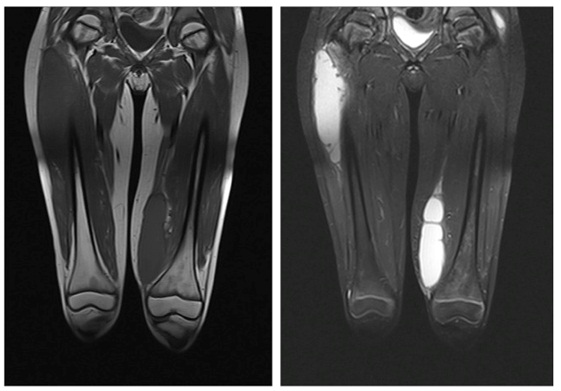
Hydatid cysts in the soft tissue of an HIV-infected child.
References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®