
Frans Radebe NICD/NHLS
A 50-year old man from Mozambique presented with a painless penile ulcer with bilateral, tender, matted inguinal lymphadenopathy that had not ruptured. His testes were normal and there was no visible urethral discharge. Genital samples were collected from the ulcer and urethra for Chlamydia culture and blood taken for syphilis and HIV serology.

Genital swab and urethral cultures were positive for Chlamydia trachomatis and Chlamydia trachomatis IgG titre of 1:256 was observed. Syphilis serology was positive at a titre of 1:2 for RPR. He was treated with doxycycline 100mg twice a day for 21 days HIV ELISA was negative. Bubo pus was aspirated from the patient post-treatment, which was negative for Chlamydia on culture. In line with syndromic management of genital ulcer syndrome, he was treated with Benzathine Penicillin for syphilis
Question 1: Discuss the aetiology and pathogenesis of LGV.
Answer to Q1
Aetiology of and pathogenesis of Lymphogranuloma venereum Lymphogranuloma venereum (LGV) is a genital infection caused by the invasive L-serovars of C.trachomatis. The disease is endemic in many parts of the tropics. LGV occurs in travelers who acquire the infection while visiting or living in an endemic area. It cannot penetrate intact skin but gains entry through minute lacerations and abrasions and is predominantly a disease of the lymphatic tissues. Patients with LGV may present with enlarged, painful inguinal lymph nodes, which may be either unilateral or bilateral. Swelling of both inguinal and femoral lymph nodes may result in the formation of a characteristic “groove-sign”. These inflamed lymph nodes may develop into buboes, which may suppurate and subsequently rupture resulting in the formation of inguinal or femoral ulcers and sinuses. Chronic lymphadenopathy with progressive tissue destruction may follow. Apart from a transient, ‘herpetiform’ primary lesion of the external genitalia or an anal ulcer, the clinical evidence of the primary site of infection is only apparent in 3% of cases at presentation. In women early disease may go unrecognized as a result of primary lesions being situated on the cervix. The vast majority of patients recover from LGV without sequelae, but the persistence of Chlamydia in anogenital tissue may cause a chronic inflammatory response and the development of genital ulcers, fistulas, rectal strictures & genital elephantiasis1-4.
In South Africa, LGV is a minor cause of genital ulcer disease, but occurs more frequently in some distinct rural regions comprising Mpumalanga, KwaZulu-Natal and the Eastern Cape with isolation rates of less than 1%.5-8 The infection is frequently detected among migrant-workers, the majority having acquired their infections from Lesotho, Botswana, Swaziland, Mpumalanga and the Eastern Cape.9 Recently, outbreaks of LGV have been reported among MSM and bisexual men many of who are HIV-infected and practice receptive anal intercourse. 10
Question 2: What laboratory tests are available for diagnosis and subtyping of LGV.
Answer to Q2
LGV is commonly diagnosed by:
Less common methods include:
Question 3: Discuss the treatment algorithm for a patient with genital ulcer and lymphadenopathy.
Answer to Q3
Treatment algorithm for Genital ulcer syndrome and antibiotic therapy for LGV
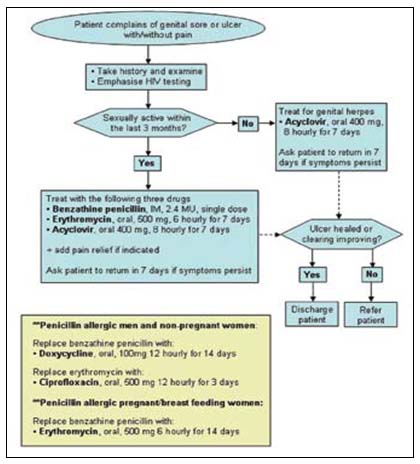
Adapted from the revised GUS flowchart of the Primary Health Care Standard Treatment Guidelines and Essential Drugs List, 2009
Antibiotic therapy for C. trachomatis infections include:
References
As illustrated in the figure below, the inguinal lymphadenopathy and ulcer were healing by seven and fourteen days respectively (see figure). They had completely healed after 21 days.
Syndromic management is at the heart of STI treatment and accepts that immediate empiric treatment of the symptoms is needed before a definite test result becomes available. Outside of an experienced clinic setting where symptoms can be correctly identified, STI management is often poor. Although LGV responds well to antibiotic treatment, if mismanaged, LGV may cause chronic or irreversible complications. LGV diagnosis may be delayed as it requires tests that are not routinely performed such as C. trachomatis serovar isolation, nucleic acid amplification tests or serology. Recent outbreaks of LGV in Europe among MSM who are mostly HIV-infected, poses a big threat to public health. There is an urgent need to identify risk factors and strengthen clinical recognition and develop point-of-care diagnostic tests for LGV infection to enhance management.
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®