Answer to Q1
This man’s presentation combined with his origin from a country endemic for human African trypanosomiasis (HAT, Figure 1) has all the hallmarks of stage II HAT secondary to infection with Trypanosoma brucei gambiense (T. b. gambiense)
Figure 1: Geographical distribution of West and East African trypanosomiasis

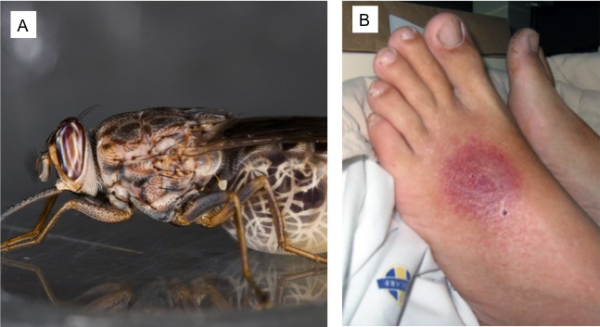
Unlike HAT secondary to Trypanosoma brucei rhodesiense (T. b. rhodesiense), which causes East African trypanosomiasis, T. b. gambiense is a more indolent infection with neurological manifestations indicative of CNS penetration by the typanosome occurring months to years after initial infection. HAT is transmitted by tsetse flies (Glossina spp, Figure 2A), and at the site of infection, a trypanosomal chancre (Figure 2B) may form after about 5 days, although this is less common in West African trypanosomiasis than in East African Trypanosomiasis. Thereafter, stage I disease follows ~2-3 weeks later in West African disease, characterized by haematolymphatic dissemination of trypanosomes, with clinical features of fever, non-specific symptoms, transient rashes and lymphadenopathy (including posterior cervical chain lymphadenopathy, first described by Winterbottom and known as Winterbottom’s sign). Hepatosplenomegaly may also be evident. Symptoms may vary in cycles of one to several days as a result of the parasite changing its variant surface glycoproteins.
Figure 2: Tsetse fly (A) and (B), a trypanosomal chancre in a patient with East African trypanosomiasis (courtesy of Prof Lucille