
Victoria Howell1, Candice Royal2, Mary Morgan2
1. Department of Microbiology, National Health Laboratory Services, Greys Hospital, Pietermaritzburg.
2. Department of Paediatrics, Greys Hospital, Pietermaritzburg
A 6-week old female infant presented to Greytown Hospital with a 1-week history of progressive respiratory distress. She was treated for 3 days with ampicillin and gentamicin but was subsequently changed to piperacillin-tazobactam and amikacin. One week after admission she was referred to Greys Hospital Paediatric ICU (PICU) because of her deteriorating condition and her need for ventilatory support.
Her mother was known to be HIV-infected and had been commenced on HAART during her pregnancy because her CD4 count was found to be 99 cells/mm3. Her routine antenatal bloods were normal and she had an uncomplicated pregnancy. She was delivered at 34 weeks gestation by normal vaginal delivery due to unexplained pre-term labour. Her birth weight was 2.42kg with Apgar scores of 9/10 and 10/10 at 1 and 5 minutes respectively. She was given nevirapine as per the PMTCT protocol. There were no complications noted during the period prior to admission. She was exclusively formula fed from birth and was growing well according to her road-to-health chart.
On admission to Greys Hospital PICU she was in respiratory distress. Her oxygen saturation was 77% and respiratory rate was 50 breaths per minute. She had bilateral crepitations and scattered wheezes. Chest X-ray showed bilateral infiltrates. She was diagnosed with bilateral bronchopneumonia complicated by ARDS and was commenced on high dose cotrimoxazole, dexamethasone, ganciclovir and meropenem on admission. On day 2 after admission it was decided that she needed to be intubated and ventilated. She was also commenced on erythromycin for a possible atypical pneumonia and fluconazole for a possible fungal infection. On day 4 her HIV PCR result was positive and she was commenced on HAART consisting of a regimen of abacavir, lamivudine and kaletra (lopinavir/ritonavir). On day 6 a repeat chest X-ray showed areas of breakdown and right lung collapse. In view of these findings it was decided to treat her with vancomycin for a possible Staphylococcus aureus infection. Her endotracheal aspirates up to this point had not yielded a positive culture.
She had no identifiable Mycobacterium tuberculosis contacts and a mantoux skin test was negative. 3 early morning gastric washings were negative for acid-fast bacilli on microscopy. On day 16 of admission superimposed nosocomial pneumonia was suspected based on her worsening clinical condition and Acinetobacter baumannii was cultured on an endotracheal aspirate. The patient was treated with ceftazidime and tobramycin based on sensitivities of the organism.
On day 18 of admission multiple abscess were noted on the patient’s left ankle, shoulder and right forearm. The lesions started as small erythematous papules that rapidly became fluctuant and then produced purulent exudates. Within 3 days of their appearance they showed necrotic ulcerative changes. X-rays of the areas were taken to exclude underlying osteomyelitis. The patient was started on intravenous cloxacillin and recommenced on meropenem but she showed no response to these antibiotics. A swab was taken from each of these sites and was sent to the microbiology laboratory. All 3 of these swabs grew an Aspergillus species that was later identified as Aspergillus flavus. The pus from all 3 lesions was negative for acid-fast bacilli on microscopy. The patient was commenced on amphotericin B. Two days later the patient was extubated and coping comfortably on nasal prong oxygen. The rest of the infant’s course in hospital was uneventful. The lesions healed slowly over the course of the next few days and no further lesions developed after the antifungal therapy was commenced. She was changed to oral voriconazole for the last 3 weeks of therapy and was discharged home on the treatment.
A urine specimen taken during the time of the manifestation of the skin lesions showed growth of Aspergillus flavus. Repeated blood cultures were negative. A 6-week culture of her endotracheal aspirate taken a week after admission was positive for Mycobacterium tuberculosis (TB). It was sensitive to isoniazid and rifampicin and first line intensive phase TB treatment was commenced.
In summary, this was an unusual case of invasive/ disseminated Aspergillus flavus in an HIV positive infant presenting with multiple cutaneous lesions with pulmonary M. tuberculosis co-infection.


Figures 1 and 2 showing the necrotic skin lesions
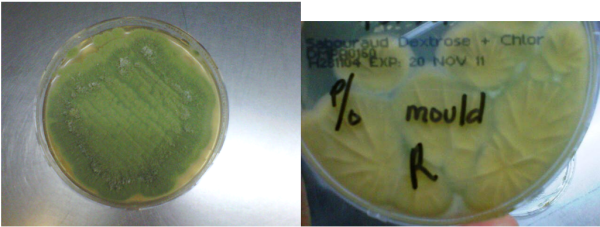
Figures 3 and 4 showing the mould growing on Sabouraud Dextrose + Chloramphenicol agar
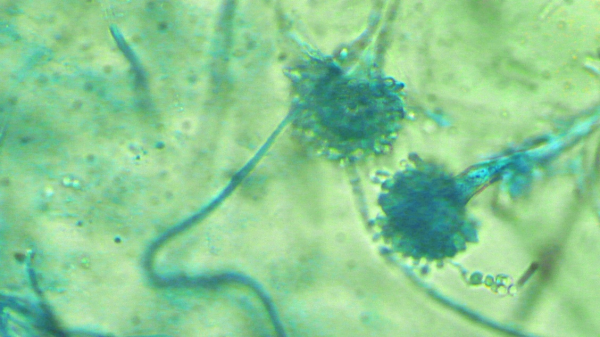
Figure 5 showing sporulating heads of Aspergillus flavus using lactophenol cotton blue stain.
ACKNOWLEDGEMENTS: Dianne Naidu from the Inkosi Albert Luthuli Hospital Mycology Reference Laboratory, Durban and the staff of Greys Hospital NHLS Microbiology Laboratory, Pietermaritzburg.
Question 1: What are the clinical features of Aspergillus infection?
Answer to Q1
The clinical features of Aspergillus spp infection are a diverse spectrum of diseases ranging from asymptomatic colonization, allergic responses, and superficial infection to acute or sub-acute invasive disease. In general, the clinical presentation is a reflection of the integrity of host’s immune system and the more immunocompromised the patient is, the greater the risk of developing invasive disease [1]. Three major clinical forms have been defined: a) Invasive aspergillosis b) chronic and saprophytic aspergillosis and c) allergic aspergillosis [1, 2].
Invasive aspergillosis frequently begins in the respiratory tract following inhalation of the conidia of Aspergillus spp, which are ubiquitous in the environment. Aspergillis fumigatus has smaller conidia (2-3m) compared to the other Aspergillus spp, which thereby enables the organism to bypass the normal host defenses in the respiratory tract and gain easy access into the alveoli[3]. Alveolar macrophages are the primary immune defense against the conidia that are deposited in the alveoli, by initiating a pro-inflammatory response that also recruits neutrophils to the site of infection. The conidia that manage to evade the host response germinate into hyphae which have the ability to elude neutrophil killing and invade the pulmonary vasculature and consequently metastasize to the rest of the body [3]. Disseminated disease is a result of either contiguous extension from the lung or the resultant haematogenous dissemination to distant sites in the body e.g. central nervous system, liver, spleen, kidney, bone and skin [1, 2].
Cutaneous infection may represent disseminated infection or may result from local inoculation of infection from a surrounding site e.g. from an intravenous catheter or an adhesive dressing. Initially there is an area of rapidly increasing erythema which subsequently develops into a necrotic, ulcerated lesion which may resemble pyoderma gangrenosum[1].
Allergic conditions include allergic aspergillus sinusitis and allergic bronchopulmonary aspergillosis. Saprophytic involvement includes aspergillus otomycosis and pulmonary aspergillomas.
Question 2: What are the risk factors for developing invasive Aspergillus infections?
Answer to Q2
Aspergillus spp have gained notoriety as an emerging cause of life threatening infections in immunocompromised patients. Risk factors include [1, 2]:
The pathological consequences differ according to the cause of the underlying immunosuppression [3]. Aspergillosis was initially included as an AIDS-defining opportunistic infection in the 1982 CDC classification [4], but was subsequently dropped due to lack of evidence that a low absolute CD4 lymphocyte count was a predisposing factor or that there was any significant increase in numbers of cases of invasive aspergillosis in HIV-infected patients [5]. HIV positive patients often have underlying neutropenia from antiretrovirals and chemotherapeutic agents and are prescribed corticosteroids for a variety of opportunistic infections and therefore have confounding risk factors for invasive disease[6]. In the earlier literature it was initially thought that HIV was not a risk factor for invasive aspergillosis but there has been an increasing number of reports of aspergillosis in HIV positive patients with low CD4 counts and no other predisposing risk factors for invasive aspergillosis [7-13]. Roilides et al found abnormalities with blood monocyte-derived macrophages in a clinical study of HIV positive children without risk factors for invasive pulmonary aspergillosis (IPA) irrespective of the CD4 count [14]. Determining the true incidence of Aspergillus spp infection in HIV positive patients is hampered by the challenges of establishing a definitive diagnosis.
Question 3: How is the diagnosis of Aspergillosis made?
Answer to Q3
The genus Aspergillus has approximately 200 species[3]. Aspergillus fumigatus is the most common species recovered from cases of invasive aspergillosis, followed by Aspergillus flavus and less commonly Aspergillus niger and Aspergillus terreus. Aspergillus flavus is able to survive at higher temperatures and is the predominant pathogen in areas with hot, dry climates[15]. Aspergillus flavus produces one of the potent hepatoxins known to man[16].
The definition for proven aspergillosis requires histopathological diagnosis of infection and a positive culture in a specimen recovered from a normally sterile site. Probable infection is defined by the fulfillment of criteria within 3 categories namely, host factors, clinical manifestations (symptoms, signs and radiological features) and microbiological evidence[2].
CULTURE: Aspergillus spp grow well on standard media used in the clinical microbiology laboratory and can be identified to species level in most routine laboratories based on the differences in colony morphology and microscopic characteristics of the fruiting structures. Confirmation of the diagnosis by culture of the organism is important in order to differentiate Aspergillus spp from other potentially invasive filamentous fungal infections.
Blood cultures are usually negative even in disseminated infection and are not a useful diagnostic modality[2]. Less than 10% of blood cultures may be positive[17]. For diagnosis of invasive pulmonary aspergillosis a bronchoalveolar lavage (BAL), transthoracic percutaneous needle aspiration or biopsy may be useful to establish a diagnosis. Direct microscopy of fluid and tissue specimens from these procedures may reveal the characteristic 45-degree angle branching septate hyphae or may grow Aspergillus spp on culture. Ideally, specimens obtained from these procedures should be cultured on fungal media for optimal growth. Results may be falsely negative in patients on systemic treatment therefore lack of a positive culture or direct smear result doesn’t rule out the diagnosis of invasive aspergillosis [2].
Cultures for Aspergillus spp in respiratory specimens or other non-invasive samples in high-risk patients, especially if obtained via BAL, can support the diagnosis of “probable” infection. However, because Aspergillus spp are commonly found in the environment and may colonise the respiratory tract without causing disease, Aspergillus spp may be cultured from patients who are not symptomatic, therefore positive cultures in patients with low risk for invasive aspergillosis should be interpreted with caution [1].
RADIOLOGY: Plain chest X-rays are of limited diagnostic utility because they lack adequate sensitivity and specificity. On CT scan of the chest the “halo sign” (an area of low attenuation surrounding a nodular lesion) and the air-crescent signs are characteristic but not diagnostic [18]. Other angio-invasive filamentous fungi e.g. zygomycetes may show similar characteristics on CT scan. These signs were initially described in neutropenic patients and may not always be evident in other immunocompromised patients with invasive aspergillosis.
Culture and identification of Aspergillus spp is the gold standard for diagnosis, but in haemodynamically unstable patients it may not be practical to perform invasive procedures to obtain a culture; therefore other markers of infection may be useful in the assessment of patients at risk for invasive aspergillosis.
NON-CULTURE MODALITIES: The serum galactomannan (GM) assay (Bio-Rad, Platelia) is a non-invasive serological assay that has demonstrated its capability in several clinical trials to be able to detect infection early in the course of invasive aspergillosis. GM is a polysaccharide that is specific to part of the living Aspergillus cell wall. The test may be falsely positive in the following cases [2]:
False positive results have been noted in children with primary immunodeficiencies notably chronic granulomatous disease[19].
Beta-1-3-D-glucan is a qualitative test that is a variation of the limulus assay used to detect endotoxins. It signifies the presence of invasive fungal infection but is not specific for Aspergillus spp. It has a sensitivity of between 64-70% and specificity of 87-90% on a single positive result. Specificity increases to >96% if 2 or more sequential samples are taken [17]. Causes of false positive results [2, 17]:
Molecular diagnostics, e.g., PCR which amplifies Aspergillus specific genes, have shown promise in some studies.
Question 4: What is the management of invasive Aspergillus infections?
Answer to Q4
Currently there are no interpretive breakpoints for any of the antifungal agents against the filamentous fungi, but the recently developed CLSI standardized methodology for antifungal susceptibility [20] represents an advance in the laboratory evaluation of Aspergillus spp.
A large randomized control trial (RCT) demonstrated that voriconazole is superior to deoxycholate- amphotericin B as primary treatment for invasive aspergillosis [21]. A RCT comparing 2 doses of liposomal- amphotericin B showed similar efficacy in both arms, suggesting that liposomal therapy may be considered as an alternative in some patients [22]. Voriconazole may be used to treat Aspergillus terreus which is intrinsically resistant to amphotericin B. Restoration of impaired host defenses is vital to improve the outcome of invasive aspergillosis.
Voriconazole (Vfend®) is a recently developed triazole antifungal agent which is formulated as either a tablet or with a cyclodextrin solution for intravenous administration [23]. Cyclodextrin is renally cleared; therefore it may accumulate in patients with renal insufficiency. Caution is advised when using the intravenous formulation in patients with renal impairment. The oral formulation has excellent bioavailability and is not dependant on the patient’s prandial state. It is widely distributed into the tissues with CSF levels reaching a level of approximately 50% of plasma levels. Voriconazole is primarily metabolized in the liver with only 5% appearing unchanged in the urine that limits its use in urinary tract infections. In adults it exhibits non-linear pharmacokinetics. It is both a substrate and inhibitor of certain cytochrome oxidases and therefore it is advisable to review the patient’s medication for potential toxic drug interactions before commencement of therapy.
Treatment of patients with invasive aspergillosis and other serious mould infections is initiated by giving a loading dose of 6mg/kg IV every 12 hours for 2 doses and then followed by 4 mg/kg every 12 hours [2, 23]. These are greater than the doses for oral treatment, which is 4 mg/kg, rounded up to a convenient pill size. The original RCT evaluated the intravenous dosing regimen, therefore it is recommended to use parenteral therapy where feasible until further evidence becomes available [2].Dosing regimens for paediatric patients differs to adults because voriconazole exhibits linear pharmacokinetics [24] and doses may need to be higher because of the more accelerated metabolic clearance [19]. A maintenance dose of 7mg/kg is recommended by some authorities to attain clinically relevant plasma levels. Voriconazole’s side effect profile is similar to the other triazole antifungals and includes:
Treatment duration varies from patient to patient and the general recommendation is to continue treatment until there is clinical and radiological resolution of symptoms which generally relates to a treatment duration of at least 3 months [19].
Other therapeutic options for invasive aspergillosis include itraconazole, deoxycholate amphotericin B, lipid formulations of amphotericin B and the echinocandins. Posaconazole has been used for salvage therapy for invasive aspergillosis.
References:
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®