
THE RETURNING TRAVELLER: CAVEATS - S Parker, G Brink
Case 1:
A 74 yr old woman consults four weeks after an extended visit to her family in the UK. Three days prior to consultation, she experienced an acute shortness of breath on getting into bed, on a background of minimal breathless on exertion, which was slowly increasing. She had no other respiratory symptoms or chest pain.
During her trip, she developed moderately severe lumbar backache with nerve root pain. She was treated by a chiropractor and given amitriptyline 10 mg nocte, but she continued to feel some minor pain.
She had an internal fixation following a fracture of her left ankle in 1999, but had been otherwise well and was not on any chronic medication. She is physically active, walking 5km three times a week and playing tennis twice a week. She was not overweight. She had never smoked and had no history of obstructive airways disease.
On examination she was not distressed but was slightly tachypnoeic on walking through to the examination room, which settled immediately one at rest. She showed no signs of anaemia and had a normal BMI. There was no evidence of cardiac failure, BP 160/80 mmHg, PR 78 in sinus rhythm, with normal heart sounds and a clear chest. Lymphadenopathy and organomegaly was absent.
Question 1: What is the differential diagnosis
Answer to Q1
Question 2: What examinations should be requested?
Answer to Q2
Further investigations revealed an Hb 11.0 (12-15) g/dl with normal red cell, white cell and platelet counts. The ferritin was raised at 184 (10 - 120) ng/ml. CXR was normal.
She was seen again one week later as she had been away. She was feeling better and an effort ECG was arranged so as to exclude any cardiac cause.
The resting ECG showed sinus rhythm at 73 bpm. There was equivocal ST segment depression in lead V6 only. Effort ECG was terminated after 1min 35s as she became acutely dyspnoeic with further ST segment changes in lead V6.
She was referred to a cardiologist for further investigation. Cardiac cause for her dyspnoea was excluded and she was eventually shown to have multiple pulmonary emboli. She was treated with subcutaneous enoxaparin and commenced oral warfarin. She made an uneventful recovery.
On taking a more detailed history an important factor emerged: she was bedridden for a period of two weeks on account of her backache. Within two days of becoming mobile she embarked on the return flight to South Africa.
Question 1: Is age alone a predisposing factor for the development of venous thrombotic events (VTE) in the traveller?
Answer to Q1
Increasing age is well recognised risk factor for VTE in the general population, even after other medical risk factors are excluded. Incidence doubles for each ten year increase in age. Amongst travelers, in an analysis by Kelman, the risk was 7.6 per million travelers < 40yr arriving in australia after a long haul flight, rising to 140 per million in those >75yr.
Question 2: What are the predisposing factors in this case?
Answer to Q2
Question 3: What is the time frame following long haul travel for VTE?
Answer to Q3
International expert opinion is that it occurs during or within four weeks of long haul travel, yet some studies use 8 weeks as the maximum. Consider travel thrombosis in those with pre-existing risk factors who undertake multiple short flights of < 3hr duration each within a three week period.
Question 4: Must the pulmonary thrombotic event (PTE) be preceded by a VTE in the lower limbs?
Answer to Q4
Nearly 90% of DVT’s are found in the leg veins. Untreated, there is up to a 25% chance of migration to the proximal lower extremity veins such as the popliteal, femoral, common femoral or external iliac veins. From proximal veins, ~ 50% risk exists of a resultant pulmonary PE if untreated. The pelvic and arm veins can also lead to PE. DVT’s of the upper limb are usually associated with indwelling venous catheters, though a condition known as Paget-Schroetter syndrome has been described in young people or athletes with a history of strenuous arm exercise.
Question 5: What are the symptoms of PE?
Answer to Q5
Depending on the size and location of the embolus, the most common symptoms are dyspnoea, chest pain, cough, haemoptysis and collapse.
Signs of massive PE are tachypnoea, hypotension, syncope, tachycardia, narrow pulse pressure, cyanosis and increased venous pressure.
Pulmonary infarction is rare, but is suggested by pleuritic pain, friction rub. There are focal parenchymal infiltrates on chest X-ray.
Question 6: What other factors predispose to a VTE in travellers?
Answer to Q6
Question 7: How long should she remain on warfarin therapy?
Answer to Q7
Standard regimes involve 3 month therapy if a known precipitant cause such as recent surgery or prolonged immobilization exists. If a cause is not found, treat for 6 months. If she plans to undertake long haul flights in the near future and the INR is well controlled, a case can be made to extend the duration of usage. If she has a recurrence the therapy is indicated indefinitely.
Case 2:
A 45 year old travel agent who is a frequent long haul traveller presents with epigastric pain four days after returning from South America. She spent ten days in South America and flew on a number of domestic flights whilst in South America. The return flight was 9 hours 40 minutes.
She reported that she was markedly breathless on exertion and perspired more than usual. Examination was normal apart from a tachycardia of 100 beats per minute. She was apyrexial and normotensive. Chest and abdominal examination was normal.
As a pulmonary embolus was suspected she was referred for a CXR, blood count and D –dimer. The blood count was normal, as was the CXR. The D Dimer was mildly elevated at 0.53 (0 – 0.5) g/mL. Further inpatient investigation did not confirm a VTE and she was discharged. Her symptoms had more or less settled prior to departure.
She was seen two weeks later two days after return from London with a recurrence of the same symptoms. As her symptoms were identical to the initial presentation it was felt it was unlikely to be a VTE given the negative findings on the previous occasion. Hyperthyroidism was suspected. Ultrasound of the thyroid gland showed a multinodular goitre. TSH < 0.01 miu />L, T4 41.2 (0-19) pmol/L and T3 26.3 pmol/L. She was started on therapy and given the all clear to fly to London, New York and Canada in ten days time, returning to South Africa from Vancouver via London after a total of seven days.
Question 1: What is the sensitivity and specificity of the D–dimer assay for VTE?
Answer to Q1
The sensitivities of the D-dimer enzyme-linked immunofluorescence assay (ELFA) (DVT 96%; PE 97%), microplate enzyme-linked immunosorbent assay (ELISA) (DVT 94%; PE 95%), and latex quantitative assay (DVT 93%; PE 95%) were superior to those of the whole-blood D-dimer assay (DVT 83%; PE 87%), latex semiquantitative assay (DVT 85%; PE 88%) and latex qualitative assay (DVT 69%; PE 75%). The latex qualitative and whole-blood D-dimer assays had the highest specificities (DVT 99%, 71%; PE 99%,69%).
The use of D-dimer is particular relevant in a situation where there is a low pretest probability of a PE. If the D-dimer is negative in such a situation, PE can virtually be ruled out.
Useful tools to assist in the probability of VTE are the following:
Wells Clinical Prediction Rule for Pulmonary Embolism (PE)
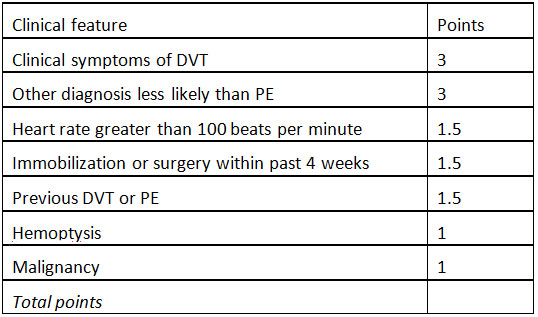
PE = pulmonary embolism; DVT = deep venous thrombosis.
Risk score interpretation (probability of PE):
>6 points: high risk (78.4%);
2 to 6 points: moderate risk (27.8%);
< 2 points low risk (3.4%)
Wells Clinical Prediction Rule for Deep Venous Thrombosis (DVT)
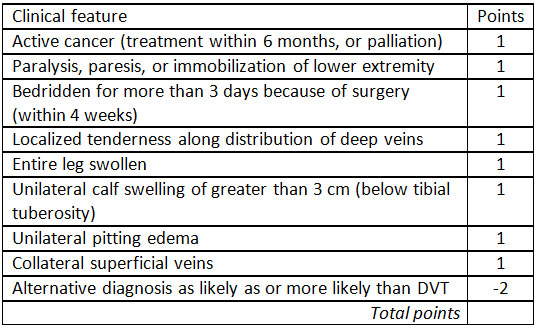
DVT = deep venous thrombosis.
Risk score interpretation (probability of DVT):
>/=3 points: high risk (75%);
1 to 2 points: moderate risk (17%);
< 1 point low risk (3%)
Question 2: What conditions results in a false positive D-Dimer test?
Answer to Q2
Elevated levels may be seen in conditions in which fibrin is formed and then broken down, such as recent surgery, trauma, infection, heart disease (including aortic dissection which can present as a PE), and some malignancies or conditions in which fibrin is not cleared normally, such as liver disease. Inflammatory conditions, pregnancy and DIC are other conditions.
Question 3: Is she at risk for VTE?
Answer to Q3
The potential serious morbidities of hyperthyroidism include ophthalmopathy, atrial fibrillation, congestive heart failure, stroke, seizure, and osteopenia/osteoporosis. Of concern would be if she were to develop atrial fibrillation and subsequent stroke whilst travelling and away. Control of the tachycardia and reduction in the T4 levels promptly would reduce the risk. Rapid control of the tachycardia and prevention of atrial fibrillation and cardiac failure can be achieved by the use of a beta blocker, such as bisoprolol, and commencing treatment with carbimazole could be considered. Ten days provides sufficient time to ascertain the benefit of the beta-blocker and her fitness to fly. Provided she is not in atrial fibrillation at the time of travel she will not be at risk for thromboembolic events.
These 2 cases illustrate the utmost importance in history taking. Patients do not know what is important in their history. In Case 1 the traveller did mention the backache but did not volunteer the information that she had remained in bed for two weeks, which undoubtedly increased her risk or PE. A family history must also be included as this can also lead one to be more specific in the differential diagnosis, thereby reducing unnecessary investigations.
A high index of suspicion in any long haul traveller presenting with an acute onset of dyspneoa of a PE is essential and should remain one of the main diagnoses to exclude. The use of the Wells predictability tables can assist markedly in deciding on the probability of either a DVT or VTE.
Careful and thorough clinical examination is critical and should not be minimized on the supposition of a likely diagnosis. Clinical signs are important. Appropriate examination in the second case would have highlighted the fine tremor in this patient and a change in the initial possible diagnosis of PTE to that of hyperthyroidism. Short cuts do not save on time or, resources and can result in greater morbidity.
References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®