
A Case Report
Theunis Avenant and Nicolette du Plessis. Paediatric Infectious Diseases Unit. Kalafong Hospital and University of Pretoria
History
A six year old girl first presented to a tertiary hospital with the complaint of headache since the age of 3 years. At times this was accompanied by vomiting. In some instances it was also associated with episodes of fever. On a few occasions she was awakened by the headache at night.
The pregnancy and birth were uneventful. Her parents are unrelated and there was nothing of importance in the family history. She walked at the age of 13 months but only spoke her first words after two years of age. There were no problems at school.
Shortly after birth she developed omphalitis. This was followed by a pyogenic infection of the skin of the neck and thighs. A chronic eczematoid dermatitis developed on the scalp. Recurrent episodes of otitis media prompted placement of tympanostomy tubes at the age of two years. Chronic suppuration however remained a problem.
Frequent episodes of lower respiratory infections necessitated regular use of antibiotics. She also had a chronic purulent nasal discharge with several episodes of sinusitis.
Secondary infections after minor trauma (e.g. clipping of nails) were quite common, with abscess formation in some cases. She had constant problems with blepharitis. Surgery was needed for a hordeolum.
Clinical examination
Her growth was still normal with both the weight and height between the 50th and the 75th percentile. Her skull circumference was 48,3cm (< P3), with brachycephaly and a sagital ridge. Her blood pressure was 115/80mmHg. A broad nasal bridge was present with deep set eyes. She had long slender fingers but flattening of the first fingers and toes. On initial clinical examination there w an eczematoid rash on the scalp with secondary infection as well as multiple palpable cervical lymph glands. The skin of the left inner thigh contained multiple small abscesses.
No hepatosplenomegaly or general lymphadenopathy was present. Neurological examination was normal and there were no signs of hypothyroidism.
Ophthalmological examination showed normal visual acuity and visual fields. No congestion was present on fundoscopy but the temporal papillae were pale.
Radiology
Conventional x-rays of the skull showed markedly increased convolutional markings (Figure 1). This was also demonstrated on computed tomography. Three-dimensional computed tomography confirmed closure of all the sutures (Figure 2). Magnetic resonance imaging revealed no intracranial pathology. Both maxillary sinuses were veiled on imaging. On chest x-ray there was atelectasis of the right middle lobe (Figure 3). This resolved with treatment, but recurred a few months later.
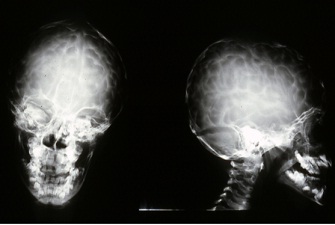
Figure 1. X-ray of skull
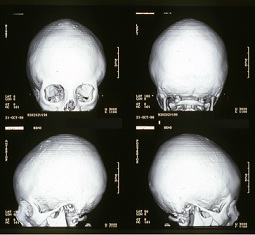
Figure 2. CT of skull
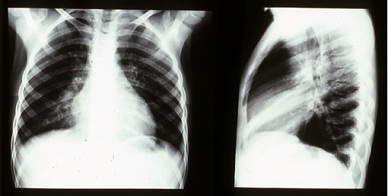
Figure 3. Chest x-ray
Blood count
| Hemoglobin | 12,5 g/dl |
| Platelets | 329 x109/L |
| Leukocytes | 9,1 x109/L |
| Eosinophils | 4,4% |
Immunoglobulin levels
| IgG | 15,40 g/L (4,78-11,29), normal subclasses |
| IgA | 1,19 g/L (0,35-1,90) |
| IgM | 0,81 g/L (0,34-1,34) |
| IgE | 5700 IU/L (< 224) igd 240 u />ml (< 100) |
Calcium, phosphate and ALP values were normal.
Granulocyte function
Slightly decreased superoxide generation. Normal chemotaxis and killing
Lymphocyte Enumeration
Normal distribution of lymphocyte subpopulations
Lymphocyte stimulation tests
Normal
On lumbar puncture the CSF pressure was normal.
A diagnosis of Hyper-IgE syndrome with craniosynostosis was made.
The disease now known as the Hyper-Immunoglobulin E syndromes (HIES) was first described by Davis et al in 1966. It was named Job's syndrome after the biblical character who was afflicted by draining skin sores and pustules.
Question 1: Which skin infections are commonly associated with primary immunodeficiencies?
Answer to Q1
Fungal infections
Candidiasis may be the first sign of an immunodeficiency. The presentation is often related to the immunodeficiency (Table 1). In patients with chronic granulomatous disease (CGD) or T-cell defects Aspergillus infections may cause erythemato-violaceous or purulent to necrotic nodular lesions. Other fungal infections may be caused by blastomycosis, coccidioidomycosis, cryptococcosis, histoplasmosis, paracoccidioidomycosis, mucormycosis or sporotrichosis.
Bacterial infections
Staphylococcus aureus is a common cause of pyogenic infections of the skin in these patients. The presentation may be atypical (cold abscesses) due to defective migration or function of neutrophils in conditions such as CGD or Hyper-IgE syndrome. Pseudomonas skin infections may be found in PID’s such as agammaglobulinaemia and may present as ecthyma gangrenosum. Pyogenic infections are also common in the Wiscott-Aldrich syndrome (WAS). This is as result of defective interaction between T-lymphocytes and antigen presenting cells.
Viral infections
In patients with T-cell deficiencies herpes virus infections (CMV, EBV, HSV, VZV) are very common. The lesions are often pronounced. Molluscum contagiosum infections are often widespread and severe. Disfigurement may occur. Epidermodysplasia verruciformis is a lifelong papillomavirus infection believed to be a consequence of an inherited cell-mediated immunodeficiency. Other manifestations of papillomavirus infections are warts and condylomata accuminata.
Table 1. Presentation of Candida infection in relation to immunodeficiency type
Question 2: What are the clinical features of the Hyper-IgE syndromes (HIES)?
Answer to Q2
Hyper-IgE syndrome is classified into two categories. Autosomal dominant HIES (AD-HIES) results from STAT3 (Signal transducer and activator of transcription 3) mutations and have abnormalities in multiple systems, including the skeletal and dental systems. Autosomal recessive HIES (AR-HIES) is a rare condition with abnormalities confined to the immune system. The rest of the discussion will be limited to AD-HIES.
Clinical manifestations
Skin
Babies may be born with, or acquire a rash shortly after birth. It typically affects the face and scalp. Biopsies show an eosinophilic infiltrate and may culture Staphylococcus aureus. So called ‘‘cold’’ abscesses demonstrate virtually no external signs of inflammation but contain frank pus from which S. aureus is usually cultured. Mucocutaneous candidiasis is a common finding.
Lung
Patients typically suffer from recurrent pyogenic pneumonias. As with the cold abscesses the symptoms are fewer as would be expected. S. aureus, Haemophilus influenzae and Streptococcus pneumoniae are commonly isolated. Pneumatocoeles and bronchiectasis frequently result from these infections.
Characteristic facies
The typical appearance develops during childhood and adolescence. Facial asymmetry with a broad nose, deep-set eyes and a prominent forehead are common.
Cranial Abnormalities
Craniosynostosis, as demonstrated in Figures 1 and 2, as well as Chiari 1 malformations may occur in Hyper-IgE syndrome. Neither usually requires surgical intervention.
Dentition
A large number of these patients retain their primary teeth past the age where exfoliation should take place. Once these teeth are removed, secondary teeth emerge.
Musculoskeletal findings
Skeletal abnormalities include scoliosis, osteopaenia/osteoporosis, frequent minimal trauma fractures of long bones, hyperextensibility, and degenerative joint disease.
Vascular abnormalities
Arterial aneurysms have recently been identified as an important abnormality associated with HIES. Management strategies however remain to be determined.
Malignancies
An increased risk of malignancies such as Hodgkin's and non-Hodgkin's lymphoma (NHL) exists.
Question 3: Which pathogens are associated with Hyper-IgE syndromes?
Answer to Q3
Pathogens associated with STAT 3 deficiency*| Frequent Pathogens |
| Staphylococcus aureus (lung and skin) | |
| Streptococcus pneumoniae (lung) | |
| Haemophilus influenzae (lung) | |
| Candida albicans (mucocutaneous) |
| Secondary Pathogens of Lung |
| Pseudomonas aeruginosa | |
| Aspergillus species | |
| Scedosporium species | |
| Nontuberculous mycobacteria |
| Less Frequent Pathogens |
| Pneumocystis jiroveci (lung) | |
| Histoplasma (gastrointestinal tract) | |
| Cryptococcus (brain and gastrointestinal tract) |
Question 4: What laboratory findings can be expected in the Hyper-IgE syndromes?
Answer to Q4
Only two laboratory findings are fairly consistent. By definition the serum IgE level is elevated. The majority of patients have levels above 2000 IU/mL. It may be as high as 50 000 IU/mL. There is a natural fluctuation in the levels that should be kept in mind. In adults the levels may even normalize, despite persistence of the clinical abnormalities. As there are other causes for a very high IgE the diagnosis must be made on a combination of clinical and laboratory findings. Eosinophilia is almost always present, but is not correlated with the serum IgE.
Other laboratory findings are variable. Total white blood cell counts are typically normal and may not increase appropriately during acute infection. Neutropaenia is uncommon. Levels of serum IgG, IgA and IgM are usually normal. Elevated IgD is known to be associated with Hyper-IgE syndrome although the significance is not clear. No specific immune defect has been consistently demonstrated in patients with HIES.
A polymerase chain reaction (PCR)–based high-resolution DNA-melting assay scanning selected exons of the STAT3 gene may establish a rapid molecular diagnosis in many patients.
Question 5: What are other causes of an elevated IgE level?
Answer to Q5
Circulating IgE levels are predominantly elevated in helminthic parasitic and allergic conditions. Table 2 provides a list of conditions in which elevated IgE levels may be found.
The only clearly identified protective role of specific IgE antibody is its role in the killing of nematode parasites. A predilection for the production of IgE in immune responses to environmental antigens (allergens) is the defining characteristic of atopy.
Less common causes include malignancies, primary and secondary immunodeficiencies, infectious diseases, inflammatory disorders and adverse drug reactions.
An elevated IgE concentration is not diagnostic of any single condition. However, there are at least 3 conditions (IgE monoclonal gammopathy, hyper-IgE syndrome, and allergic bronchopulmonary aspergillosis) in which elevated IgE levels are universally observed.
Winter WE et al.Arch Pathol Lab Med—Vol 124, September 2000, 1382 -1385
References
No definitive therapy is available for the treatment of hyper-IgE syndrome. The patient was placed on antibiotic prophylaxis and the craniosynostosis was managed conservatively with regular clinical and ophtalmological follow up.
Recurrent or chronic skin infections are clues that may aid in the diagnosis of primary immunodeficiencies. In some cases it can even help in coming to a specific diagnosis. Syndromes such as HIES are multisystem disorders and associated abnormalities should actively be sought for.
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®