October 2010
Moherndran Archary, Ashendri Pillay, Raziya Bobat
Paediatric Infectious Disease Unit, Department of Paediatrics and Child Health University of KwaZulu Natal
In July 2010, a 6 year old HIV positive male child on HAART since June 2008 with immune restoration, presented to an emergency paediatric unit in Durban, with fever & headache of 1 week duration.
His immunisations were complete according to the South African vaccination schedule prior to 2009. He resides in KwaZulu Natal with his grandmother under poor social circumstances.
No prior history of head trauma or rhinorrhoea was noted
On examination he was pyrexial with a temperature of 38oC.
CNS examination revealed photophobia and neck stiffness with positive Brudzinski & Kernig signs. He had a normal level of consciousness.
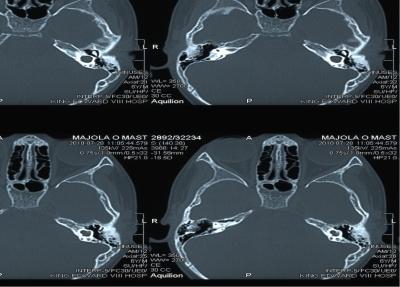
A mildly inflamed left tympanic membrane was noted on ENT examination.
A primary diagnosis of meningitis was made & the relevant investigations carried out:
His full blood count revealed a WCC of 25 x 109/L, platelets 341 x 109/L, Hb 13 g/dL, a normal U&E and a mildly elevated globulin level of 43g/L on his liver function tests
HIV viral Load was undetectable & his CD4 was 308 cells/mL
CSF Biochemistry
Protein 2.60
Globulins +++
Chloride 112
Glucose 0.2
CSF MC&S
PMN 260
Lymphocytes 64
Erythrocytes 120
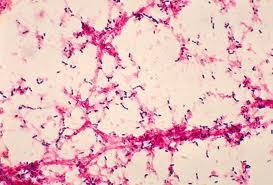
Gram positive cocci on CSF
Gram positive cocci on blood culture (figure 1)
Streptococcus pneumoniae identified on blood & CSF cultures
Both sensitive to Ceftriaxone
Figure 1. Blood culture showing Gram positive Streptococci