
Dr Andrew Whitelaw, President of the Infection Control Society of Southern Africa.
With acknowledgments to Sr C Rinquest, Dr J Wojno and Dr V Madikae who have been involved in the ongoing investigation of the outbreak.
The cardiac surgeons inform you, the infection control practitioner, about a possible outbreak of Staphylococcus aureus post-operative wound sepsis. In the last 2 months, 6 patients have developed S. aureus sepsis post operatively. They now contact you to demand that you investigate the outbreak, that you swab every staff member and patient, as well as testing the operating theatre for contamination.
A summary of the cases is as follows:
Case 1: Surgeon Dr A; assistant Dr Z, anaesthetist Dr G
Superficial wound sepsis 1 week after surgery. S. aureus (cloxacillin resistant) isolated from wound swabs.
Case 2: Surgeon Dr B, assistant Dr Z, anaesthetist Dr F
Deep surgical site infection and septic pericarditis 10 days post-operatively. S. aureus (cloxacillin susceptible) isolated from pericardial fluid and blood cultures.
Case 3: Surgeon Dr A, assistant Dr Z, anaesthetist Dr F.
Deep surgical site infection about 3 weeks post operatively. S. aureus isolated from tissue, resistant to cloxacillin.
Case 4: Surgeon Dr C, assistant Dr X, anaesthetist Dr G
Deep surgical site infection and S. aureus bacteraemia 6 days after surgery. S. aureus susceptible to cloxacillin
Case 5: Surgeon Dr B, assistant Dr X, anaesthetist Dr E
Deep surgical site infection 4 days post operatively. S. aureus isolated, sensitive to cloxacillin.
Case 6 Surgeon Dr C, assistant Dr Z, anaesthetist Dr B
Deep surgical site infection 17 days post operatively. S. aureus (cloxaciliin susceptible) isolated from swabs.
Three of the isolates were available for molecular analysis, and the result is shown below.
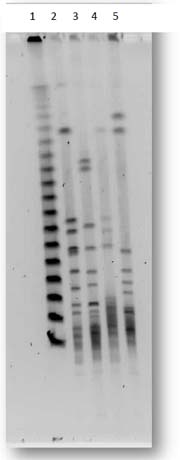
Pulsed field gel electrophoresis of S. aureus genomic DNA digested with SmaI
Lane 1: MW marker
Lane 2: NCTC 8325 (ref strain)
Lane 3: Isolate from Case 2
Lane 4: Isolate from Case 4
Lane 5: Isolate from Case 5
Question 1: What are the basic principles involved in investigating an outbreak such as this?
Answer to Q1
The following is a general guide to the steps that are involved in an outbreak investigation. Although they are presented in a sequential fashion, many of the processes may run concurrently. These steps are designed to illustrate general principles rather than the investigation of the specific outbreak described above. However, where relevant, the outbreak in the case is referred to.
Question 2: What is the role of strain typing in nosocomial outbreaks?
Answer to Q2
Strain typing is performed in order to determine whether the organisms involved in an outbreak are all identical or not. There are a number of ways of determining if the strains are related. The easiest is to examine the antimicrobial susceptibility patterns. However, while easy, this is not a very reliable method as identical strains do not always share identical susceptibility profiles. The interpretation of differences in the antimicrobial susceptibility profile (the antibiogram) depends partly on which antibiotics have different results, and also on how many different agents show differences between strains. In this case, since there is a mixture of MRSA and MSSA isolates, it would seem unlikely that the strains are identical, but further confirmation would be preferable. Conversely, unrelated strains may have very similar or identical antibiograms, and finding MRSA in every patient would not on its own prove a common source outbreak.
Molecular typing has become more and more widely used for this purpose, and there are multiple methods for doing this. Pulsed field gel electrophoresis (PFGE) is still regarded as the gold standard; however it is labour intensive and time consuming. PCR based methods, while not always as discriminatory, are often quicker and easier to perform. Some of the PCR based methods include randomly-amplified PCR (RAPD), PCR plus sequence analysis of specific regions (such as spa-typing), or PCR with analysis by restriction fragment length polymorphism (RFLP). Obviously the major limitation of molecular typing is the need for the isolates, and in many cases, some isolates are not available as the cases are only recognised as being part of an outbreak days or weeks after culture results are available, as was the case in this outbreak.
The significance of an outbreak involving identical strains does depend in part on the nature of the outbreak and the timing of the outbreak. In the case presented above, if all the S. aureus isolates had been identical, it would suggest introduction of the organism from a common source – such as a health care worker carrying that strain, or an environmental source that all patients had been exposed to.
The PFGE electrophoresis performed on the three available isolates from this case show that the isolates are not, however, related. Using the Tenover criteria (Tenover at al, 1995) the 3 strains exhibit more than 7 DNA band differences with one another. This 7 band difference corresponds to 3 or more independent genetic events in these strains that make them different.
The fact that the S. aureus isolates are unrelated implies that the patients are being exposed to a variety of organisms. This could either be the patients’ own flora which are causing infection due to a breakdown in some infection control practice (such as failure of pre-operative skin preparation), or the organisms could be originating from a variety of external sources, but are causing infection due to (again) a breakdown in infection control practice, such as inadequate cleaning and sterilisation of the surgical instruments.
Question 3: What is the role of environmental sampling in investigating nosocomial outbreaks?
Answer to Q3
Environmental sampling involves taking specimens from items in the environment that may be implicated in spread of organisms. Sampling can either be done to identify a common source outbreak (for example sampling intravenous fluid or food samples to determine whether they are contaminated, or testing health care workers for carriage of MRSA), or sampling can be done to determine whether an environmental control has malfunctioned (for example air sampling in an operating theatre to determine whether air quality is at fault due to poor maintenance of air conditioners).
Environmental sampling is usually only of value if it is directed by a hypothesis, or is based on some knowledge of the spread of the organism involved. Thus, in a suspected case of food poisoning, sampling the suspected food makes sense. Similarly, in an outbreak of Legionnaire’s disease, it may appropriate to sample the water supply. However, in an outbreak of nosocomial infection due to a multi-resistant Gram negative bacillus, some epidemiological investigation should be conducted first to identify possible common associations which could then be used to direct environmental sampling.
Environmental sampling is not always reliable – absence of a positive culture from an environmental sample does not necessarily disprove the hypothesis that led to that sample being taken, and presence of a positive culture from the environment does not necessarily confirm that environmental source as being responsible for the outbreak. Environmental cultures must be backed up by reliable epidemiological data. This need for caution often needs to be balanced by the need to investigate an outbreak as quickly as possible, as well as the fact some environmental sources may need to be sampled before they are lost (such as food, medication vials). Therefore it may prudent to collect potentially important environmental samples quickly, but delay microbiological processing until more information is available to allow one to only test a proportion of the collected samples.
In the case in question, since the infecting isolates were unrelated, we felt that it was not necessary to screen HCWs for carriage, nor was it necessary to try to identify a common environmental source by “swabbing the entire theatre” (as requested by one of the clinicians). We did attempt to perform air sampling in the theatre and set-up areas using settle plates. While the best method of air sampling is by use of a dedicated air sampler, this equipment is not widely available. Settle plates involve placing an agar plate in the environment, open, for a period of an hour, and then incubating to determine how many colony forming units (cfu) are present. It is probably best to do this while the theatre is in normal use to reproduce normal conditions as much as possible; in this case the theatre had already been closed, so the settle plates were testing an empty theatre which is less ideal. The settle plates in this case all cultured less than 4 cfus, which is considered acceptable for an operating theatre at rest.
Question 4: How useful is pre-operative screening and/or decolonisation in preventing S. aureus surgical site infection?
Answer to Q4
A number of studies have evaluated the efficacy of intranasal mupirocin prior to admission or prior to surgery as a means of reducing post operative infections. While not all studies have been randomised trials, and the methodology and interventions have varied, there does appear to be a consistent reduction in surgical site infections in patients who receive intranasal mupirocin prior to surgery, although the effect is most marked in cardiothoracic and orthopaedic patients. A review and meta-analysis from 2005 (Kallen et al) reviewed 7 eligible publications assessing the impact of intranasal mupirocin pre-operatively. Although there was no significant reduction in risk of post operative infection in patients undergoing general surgery, there was a significant reduction in infections in patients undergoing cardiothoracic and orthopaedic surgery. The relative risk (RR) for cardiothoracic surgery was 0.37 (95% CI: 0.25-0.55) based on two non-randomised “before and after” studies, and was 0.69 (0.46-1.03) for the one randomised trial included in the review.
A more recent randomised controlled trial published in 2010 (Bode et al) randomised 907 medical and surgical patients proven to be S. aureus carriers to either S. aureus eradication or placebo. The eradication arm consisted of intranasal mupirocin as well as chlorhexidine washes for 5 days. Of the 907 patients, 808 underwent surgery. There was a reduction in deep surgical site infections in the intervention arm, with a RR of 0.21 (95% CI: 0.07-0.62). The reduction in superficial infections was less marked, with a RR of 0.45 (0.18-1.11).
The other question revolves around the value of pre-admission screening specifically for MRSA carriage, and is possibly more difficult to answer. A review of the literature by McGinigle in 2008 found very few well conducted studies that have evaluated this question. While many of the studies reviewed did show an impact of routine MRSA surveillance cultures, the methodology in all of them was suboptimal, and there were no randomised controlled trials. The additional question of the cost-benefit of this approach has yet to be adequately addressed. In 2008, Jeyaratnam et al conducted a cluster randomised study comparing the effect of a rapid PCR based screening for MRSA with traditional culture based methods. While the PCR-arm showed a reduction in reporting time and reduction in unnecessary isolation days, there was no reduction in MRSA acquisition rate between the two groups. The British Society for Antimicrobial Chemotherapy Guidelines for MRSA control do advocate routine screening of patients for MRSA, but advise that it only be performed on targeted patient populations, and only if interventions / facilities to isolate carriers are available.
Likewise, the practice of routine screening of staff members remains controversial. While it may be appropriate to screen HCWs in the face of an outbreak of MRSA, since it is known that HCWs (and patients) can be carriers of MRSA and thus serve as a potential source, the value of pre-employment screening and eradication is less clear. This is partly due to the costs and logistical difficulties involved in doing this, and partly due to the fact that many people may become re-colonised after de-colonisation and that colonisation may be intermittent. The BSAC do not recommend routine staff screening, unless it is in the face of an outbreak of MRSA.
Thus, while the evidence does seem to favour preoperative S. aureus eradication for reduction of post-operative surgical site infections in selected surgical patients, the value of routine screening of all patients for MRSA as an infection control intervention is possibly more controversial. Routine screening of some or all patients for MRSA carriage pre-supposes that facilities and resources exist to actively intervene in some way when patients are identified as carriers. This is often not the case in many health care facilities in South Africa.
References:
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®