
Eiman Alblooshi, Pediatric infectious disease fellow, UKZN
Reviewed by Prof. Moherndran Archary, UKZN.
B.A is a 12-year-old boy, living with HIV and virologically suppressed since 2020 after being changed to a Dolutegravir based antiretroviral therapy regimen. He was started on ART in 2012, with a long history of prior immunological and virological failure. He presented to the hospital with a 4-day history of vomiting, headache and blurred vision.
In Emergency Department: he was febrile, tachycardic and drowsy. His Glasgow Coma Scale was 10/15. He had neck stiffness with positive Kernig’s sign.
Considering the clinical picture of fever associated with neurological deterioration and meningitic signs, a meningitis was high on the list of differentials.
Laboratory results:
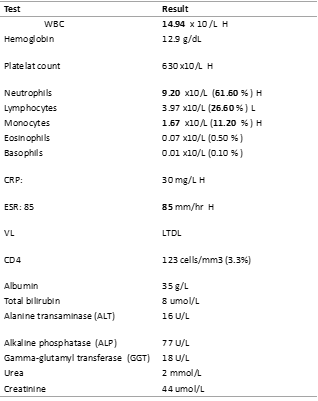
Lumbar puncture results:
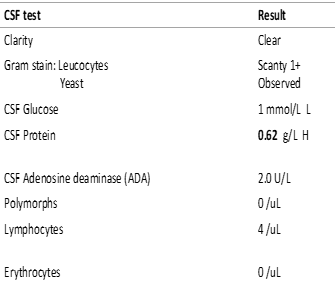
The results confirmed the diagnosis of cryptococcal meningitis (CM) in this patient.
B.A received 2 weeks of Amphotericin B deoxycholate and fluconazole (flucytosine was not available). He improved clinically and discharged home to continue fluconazole at a dose of 6mg/kg/day.
B.A presented to the hospital after 4 weeks with fever, severe headache, photophobia and neck stiffness. His physical examination was showing signs of meningitis. The family reported adherence to current treatment.
A lumbar puncture was repeated and showed the following results:
On repeated Labs: CD4 count : 540 cells/mm3 (26.6%) , HIV VL: LTDL
CSF culture from the first admission was reviewed and cultured Cryptococcus gatii and Cryptococcus laurentii.
Differential Diagnosis:
The possible differential diagnosis for CM Symptomatic relapse include:

Management
The management of cryptococcal meningitis is divided into 3 phases:
Combination antifungal therapy has improved outcomes and antifungal monotherapy should be avoided. Flucytosine containing treatment regimens have higher survival rates. Cryptococcus species are intrinsically resistant to Echinocandins (echinocandins).
World Health Organization (WHO) guidelines:
https://www.who.int/publications/i/item/9789240052178
Final diagnosis
Can cryptococcal meningitis occur in virally suppressed patient?
Yes, because the risk factor to develop Cryptococcal meningitis is not the presence of an HIV infection, but a low number of CD4 T-cells (increasing risk when CD4+ < 350/mm3).
Cryptococcal meningitis can accur in:
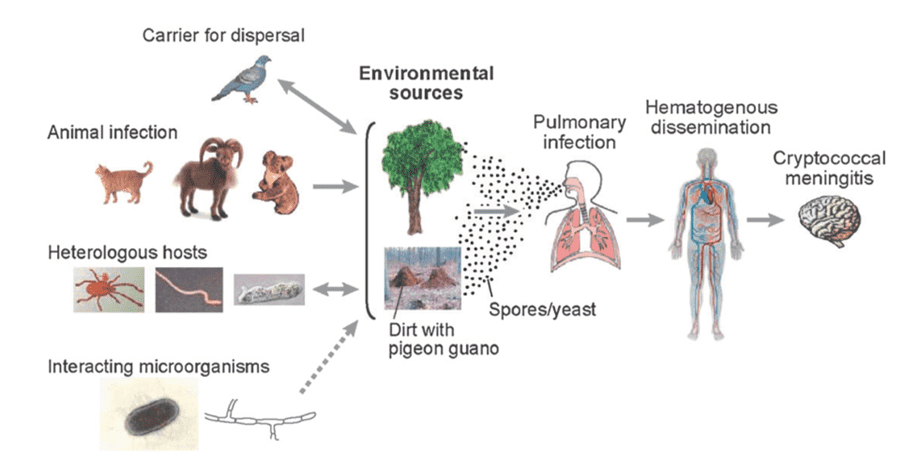
Cryptococcus lives as a yeast in the environment. Humans and animals can become infected after inhaling airborne, dehydrated yeast cells or spores, which travel through the respiratory tract and enter the lungs. The environment inside the host body signals the progression of the infection to disseminate and infect other organs like CNS.
Our patient showed a viro-immunological discordance (supressed viral load with low CD4 count). These immunological discordant responses among people living with HIV have reported in 13 to 29% of patients.
The risk factors for viro-immunological discordance are:
Discordance response increases the risk for:
Cryptococcus gatii and Cryptococcus laurentii.
The major pathogenic species in the genus Cryptococcus are Cryptococcus neoformans and Cryptococcus gattii. Previously, C. gattii infection was restricted to tropical and subtropical regions. However, outbreaks have been recorded in North America. C. gattii shows higher level of heteroresistance to fluconazole compared to C. neoformans.
Cryptococcus species other than C. neoformans and C. gattii were previously considered to be non-pathogenic to humans; however, opportunistic infections associated with rare Cryptococcus spp., such as Cryptococcus laurentii and Cryptococcus albidus, are increasingly being reported.
C. laurentii has been reported that is has various levels of fluconazole resistances.
Does our patient need a change of his management in the second admission?
C. laurentii infections are rare and a standard treatment has not yet been established.
NIH Guideline for adults and adolescents with cryptococcal meningitis relapse recommend the following:
Does our patient has IRIS?
Although the patient was virologically supressed upon initial admission, his initial CD4 count was low showing viro-immunological discordance. After cryptococcal meningitis treatment the CD4 count improved. The temporal association of clinical deterioration with immune reconstruction in absence of microbiological relapse indicating paradoxical IRIS.
Immune Reconstitution Inflammatory Syndrome (IRIS) refers to a collection of inflammatory disorders, predominantly related to infectious processes that manifest after the initiation of antiretroviral therapy (ART) and can be classified as unmasking or paradoxical.
Common Scenarios of HIV Immune Reconstitution Inflammatory Syndrome (IRIS)
“Unmasking” IRIS
“Paradoxical” IRIS
References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®