
Prof NM du Plessis
Dr M Verster (Paediatrician, Cintocare hospital, Pretoria)
JM, a previously healthy 8-year-old boy, was admitted in late-April 2021 with a necrotic lesion invading his right orbit.
His symptoms started in October 2020. After a swimming lesson, his parents noted a small black lesion under his right eye (just underneath the area that the swimming goggles would normally cover). They assumed that he injured his face in the swimming pool. The lesion did not resolve, and grew larger over a period of 1 month. They did not report any fever or weight loss at the time. Nasal congestion was reported intermittently during this period.
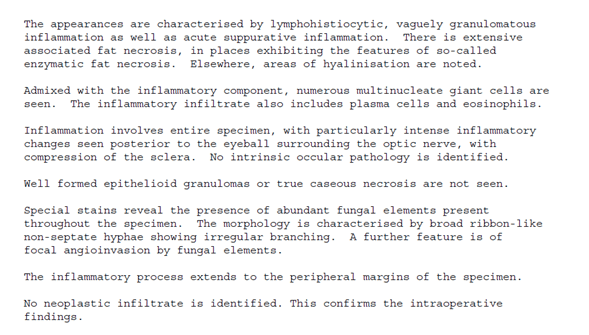
A skin biopsy was done in November 2020, and repeated in January 2021. The biopsies showed a vaguely granulomatous inflammatory process.
The differential diagnosis of an invasion granulomatous skin lesion can include a number of etiologies:(1)
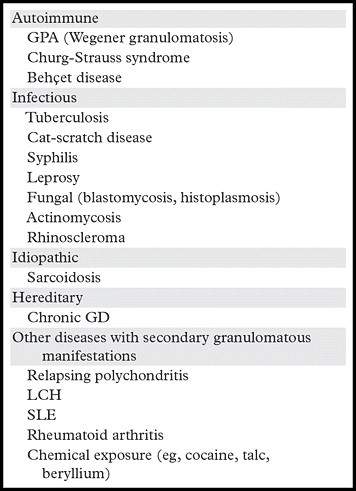
GPA = granulomatosis with polyangiitis, LCH = Langerhans cell histiocytosis, SLE = systemic lupus erythematosus.
Master JM was started on oral Fluconazole and Co-amoxiclav, but the lesion grew aggressively and started involving his right orbit. He also developed significant submandibular and cervical lymphadenopathy. He was subsequently referred to an oncologist for further management. Chemotherapy treatment for suspected Langerhans Cell Histiocytosis (although immunophenotyping remained inconclusive) was initiated by the oncologist, but without clinical improvement. At the time of his referral, he had complete destruction of the right orbit with loss of vision in his right eye (Figures 1-3 show the progression of the lesion).

Figures 1-3: The pictures illustrate the progression of the lesion under the right eye (from left to right) (Written permission given by the parents)
The following laboratory tests were performed
|
Test performed |
Reference ranges |
Results |
|
Haemoglobin |
11.5 – 15.5 g/dL |
9.6 |
|
Haematocrit |
0.35 – 0.45 L/L |
0.28 |
|
Platelets |
150 – 450 x 10^9/L |
416 |
|
Leucocyte Count |
5.0 – 15.0 x 10^9/L |
5.78 |
|
Neutrophils |
1.5 – 8.0 x 10^9/L |
51.0% 2.95 |
|
Lymphocytes |
1.5 - 7.0 x 10^9/L |
37.0% 2.14 |
|
CRP |
< 4.1 mg/L |
17.3 |
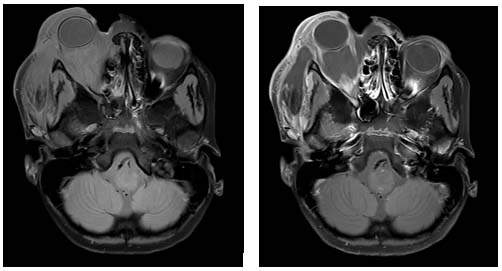
Figures 4&5: MRI brain and orbits pre-surgery (Written permission given by the parents)
There is a heterogeneous intermediate signal intensity lesion demonstrated in the right orbit.
The lesion extends from the infraorbital area, at the level of the mandible. Medial extension deforms and displaces the right nostril. There is lateral extension to the zygomatic arch. Further superior extension of the lesion is noted into both the intra- and extraconal spaces of the orbit.
Review of the previous biopsies showed the presence of numerous fungal elements.
C. gattii is a basidiomycetous fungus found in the environment. In the current HIV-pandemic, C. neoformans has been regarded as the more prevalent fungal infection causing cryptococcosis. This case gives us the opportunity to gain knowledge regarding the difference in presentation and management of the less common C. gattii, an important emerging fungal pathogen that also affects immunocompetent individuals. There are limited data available regarding the incidence of C. gattii in South Africa as well as the incidence in the HIV infected compared to the HIV uninfected population. One South African study in Gauteng that looked at cryptococcal infection during the 2002-2004 period, reported that only 2.4% of cases of cryptococcal meningoencephalitis could be ascribed to C. gattii. Of these patients, the majority (61%) was found to be HIV infected, 37% had unknown HIV status compared to 2.2% that was confirmed HIV negative (Morgan et al). Another South African study that observed cryptococcal infections in the paediatric population found that children were significantly more likely than adults to be infected with C. gattii, 9 vs. 3% (Meiring et al). Important to note however, is the prevalence of C. gattii might be higher than currently estimated since the laboratory diagnosis of C. gattii can be challenging (See laboratory aspects of Cryptococcus identification, below).
What is the natural reservoir of C. gattii?
Urgent surgical debridement and biopsies were done shortly after admission. JM required extensive surgery to remove the necrotic tissue and his right orbit was not salvageable.
The fungus was confirmed to be of the Rhizopus species, causing rhinocerebral mucormycosis. Fungal elements were subsequently also identified in the right orbit and in the bony region of the maxillary sinus:
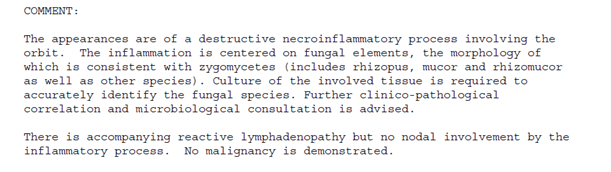
Cutaneous mucormycosis, likely Rhizopus species, with orbital invasion and destruction
Further work up did not identify a clear underlying cause for his invasive fungal infection:
High dose intravenous Amphotericin B was continued for 8 weeks, followed by a 6-month course of oral posaconazole.
JM has recovered and has gone back to school. The vision in his left eye remains unaffected.
Mucormycosis is an angioinvasive fungal infection, due to fungi of the order Mucorales. These molds live throughout the environment. The prevalence of mucormycosis in India is about 80 times the prevalence in developed countries, being approximately 0.14 cases per 1000 population. (2) Cutaneous mucormycosis is the third most common clinical type of mucormycosis. The signs and symptoms vary widely, and it is important to make the diagnosis as early as possible in order to achieve a better outcome.
The most common risk factors/predisposing conditions include:
Increasing cases of rhino-orbital mucormycosis in people with COVID-19 were recently reported, especially from India. Diabetes was present in 80% of cases, while corticosteroid treatment was given for COVID-19 in 76.3% cases. (3)
Due to the histological evidence of a “vaguely granulomatous inflammatory process”, the initial diagnosis of Langerhans cell histiocytosis was made. Langerhans cell histiocytosis (LCH) is a rare clonal disease of the monocyte-macrophage system characterized by uncontrolled proliferation and accumulation of CD1a+/CD207+ dendritic cells (DCs) as a result of continuous immune stimulation. Langerhans cell histiocytosis can occur at any age. However, peak occurrence occurs between 1 and 4 years of age. The diagnosis of LCH is based on histological criteria established by the Histiocyte Society in 1987. To make a diagnosis, it is necessary to perform a histological examination with immunophenotyping. The most frequent presenting signs and symptoms of LCH include painful bone lesions and rash. Often non-specific symptoms become prominent, such as fever, poor appetite, weight loss, fatigue, irritability and changes in behaviour. In the youngest children, the disease is often an multisystem disease with fever and symptoms of failure in various organs. In a Japanese study, the patients with skin lesions were younger than those with bone lesions. In a previous French study, 77% of the patients with the skin lesion were less than 1 year old. Sometimes there are superficial ulcerations of the lesions accompanied by oozing as the result of secondary processes leading to a bacterial superinfection. Ulcerative lesions behind the ears or involving the scalp, axillae, genitalia, or perianal region are often misdiagnosed as bacterial or fungal infections.
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®