
Sharon Elizabeth Sunny, MBChB, FCP (SA), MMed
Jeremy Nel, MBChB, FCP (SA), Cert ID (SA), MMed, DTM&H
Division of Infectious Diseases, Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
Case presentation
A 47-year-old HIV-infected female presented to a Johannesburg hospital at the end of May 2020 complaining of a 7-day history of fever, productive cough, right sided pleuritic chest pain and vomiting. She had been diagnosed with HIV in 2016 and has been on a fixed dose combination of tenofovir, lamivudine and efavirenz with cotrimoxazole prophylaxis since then. She had no history of prior opportunistic infections, including tuberculosis.
On further questioning, her sputum was white with no blood, but she did note a salty taste to it. She has had no recent travel history, no exposure to pets or wild animals and resided in Johannesburg with her family in a house with access to basic amenities.
On examination the patient appeared generally well. Her blood pressure was 105/60 mmHg, pulse 110 bpm, temperature of 37.6°C and respiratory rate of 22 bpm.
A respiratory exam revealed she was comfortable on room air; she had no chest wall tenderness. She was dull on percussion in the left upper and lower zones of the chest and right lower zone of the chest. On auscultation of her chest, she had reduced breath sounds in the left upper and lower zones as well as the right lower zone. The cardiovascular, abdominal and neurological examinations were unremarkable.
Initial investigations
Chest X-ray
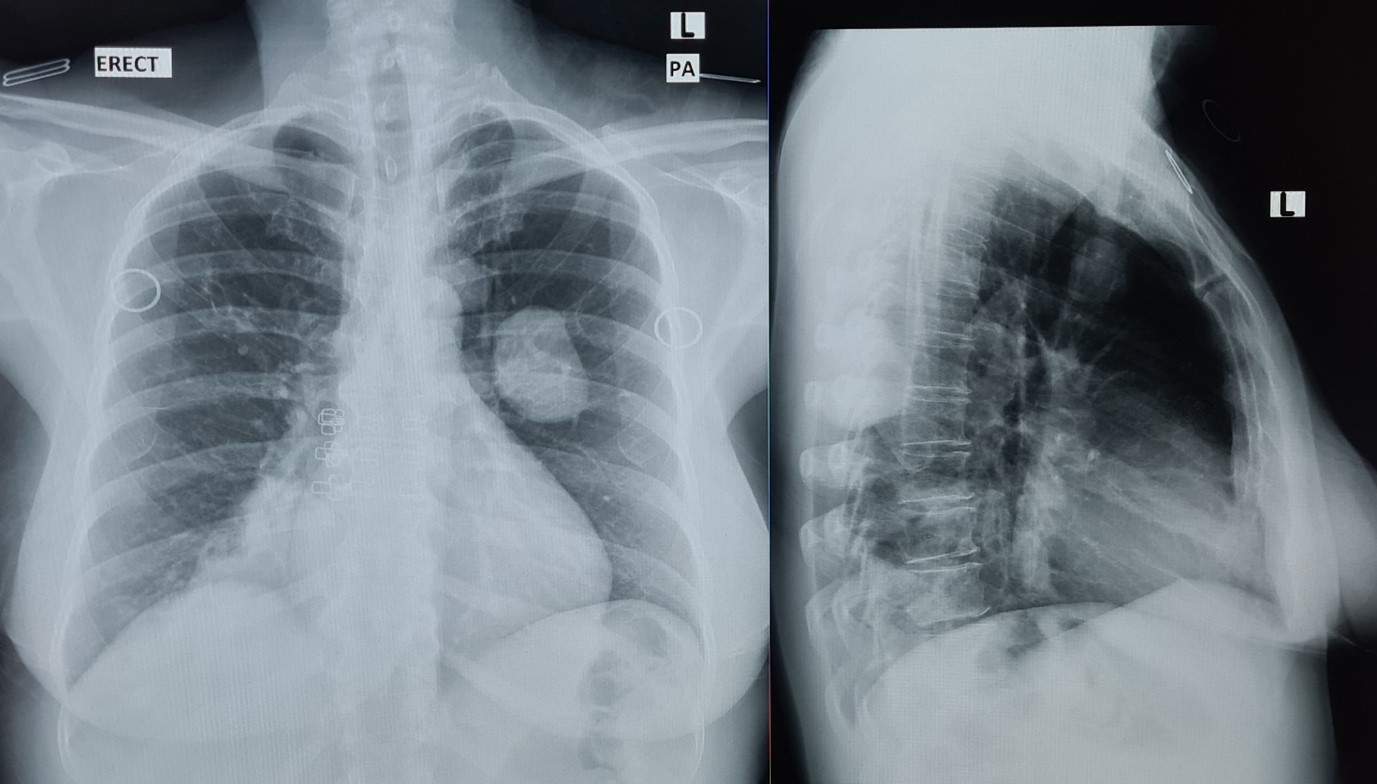
Figure 1: The patient’s chest X-ray taken in the standing position with a PA and lateral view.
Blood Investigations
Sputum Investigations
Gram stain
A CT-chest was ordered in light of the findings and additionally an echinococcus serology was requested.
Infectious differential diagnosis for round lesions on chest X-ray
1. Acute bacterial infections such as Streptococcus pneumoniae, Klebsiella pneumoniae and Hemophilus influenza can present as a “round pneumonia”, however lesions may not be multiple and as homogenous, as in this case. Air bronchograms would be expected.
2. Mycobacterium tuberculosis however symptoms are of an acute nature and no other associated features such as parenchymal involvement or pleural effusions are noted.
3. Pulmonary hydatid: Lesions are typically homogenous and are multiple. Pulmonary lesions more than 2cm are consistent with echinococcal lesions.
4. Pulmonary cryptococcal disease: Nodules are multiple and homogenous and tend to be distributed in the upper and mid zones. This patient’s chest X-ray shows 3 distinct lesions.
5. Septic pulmonary emboli however lesions are too large for emboli and this patient’s cardiovascular examination was normal.
Additional Investigations and management:
CT chest:
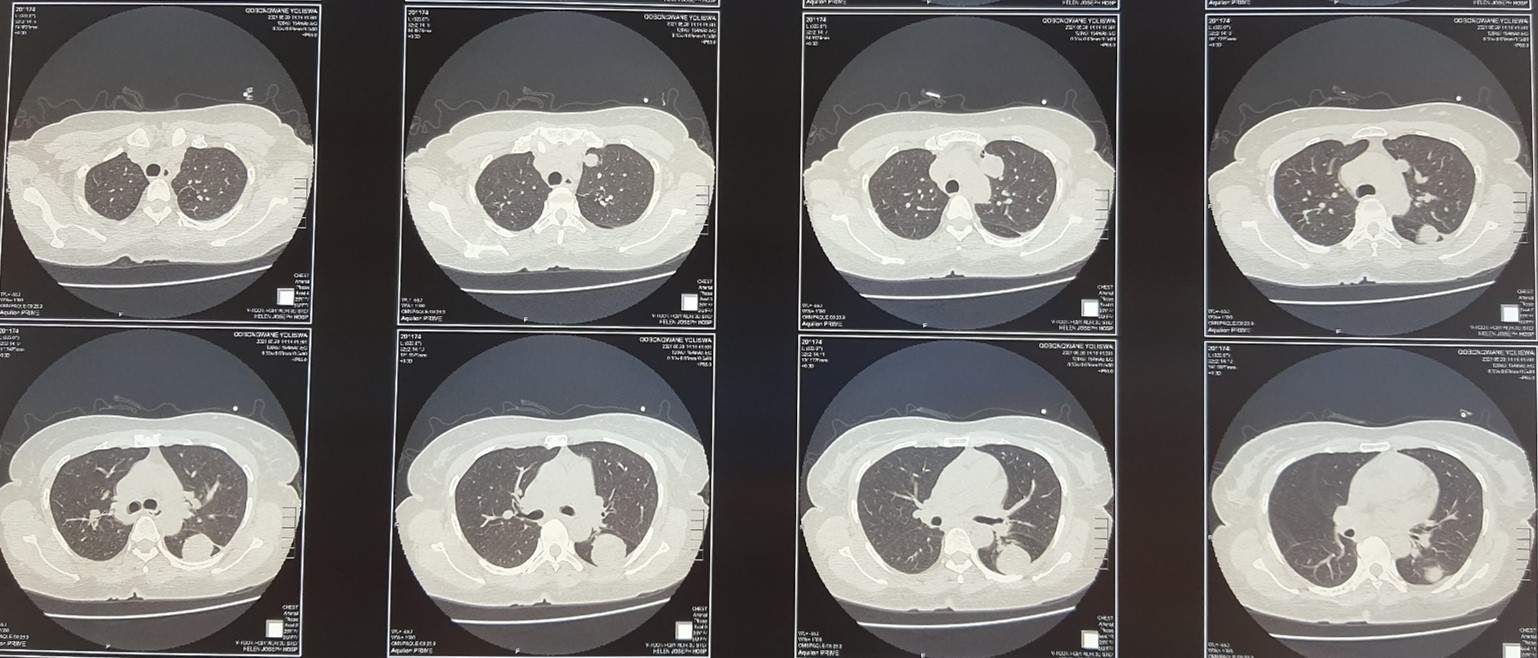
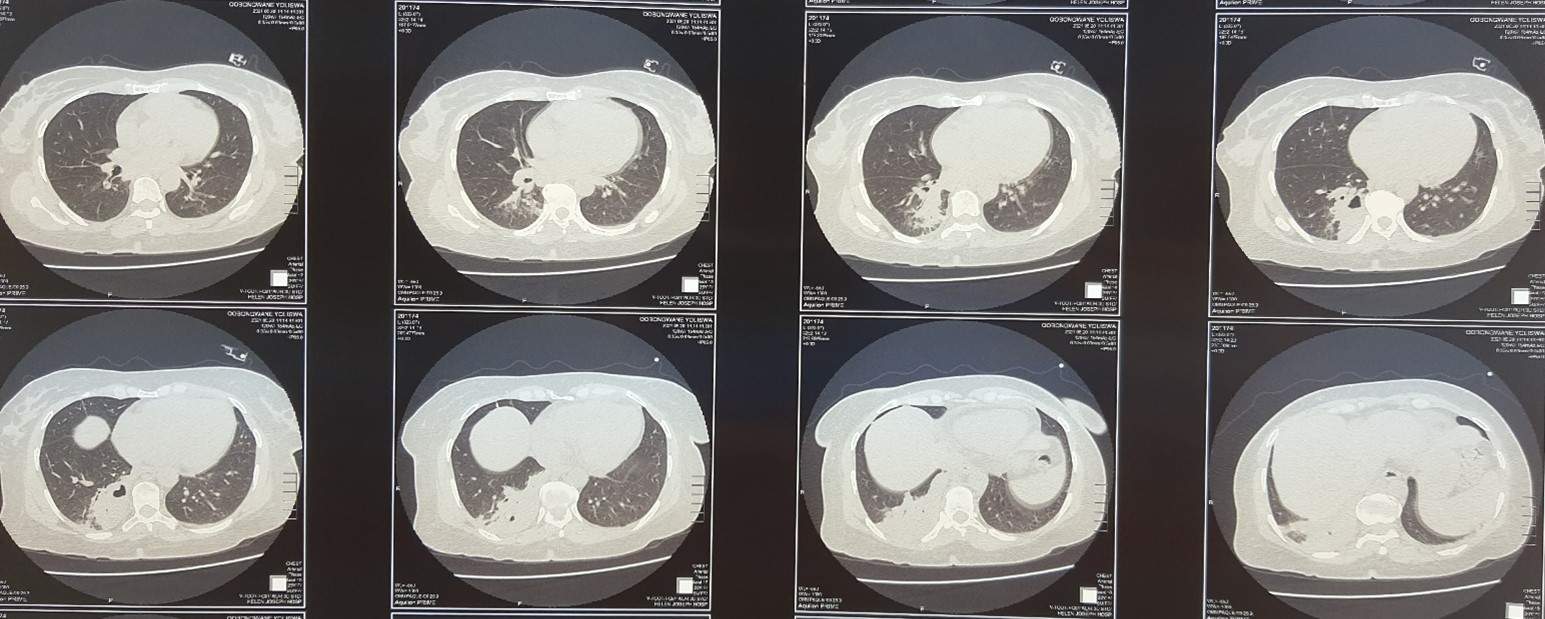
Findings :
Two left lung well defined cystic lesions with smooth contours with homogenously hypodense fluid.
= Left upper lobe: 17.8x21.4mm
= Left lower lobe: 32.5x32.2mm
Right lower lobe: 34.1x23.2mm lesion with an air fluid level and surrounding pneumonitis.
Hydatid ELISA IgG positive, 4.3u/L
Abdominal ultrasound: showed no hepatic, pancreatic or splenic cysts.
In light of the above findings, our patient was started on medical management as she had multiple cysts in more than one lobe, all were reasonably small (<3.5cm), and none of the cysts were close to any vital structures. She was commenced on albendazole 400mg po bd and the plan was to continue treatment medically until resolution of the cysts based on imaging every 6 to 12 months. 6-12 monthly imaging will then be continued up to at least 5 years from diagnosis, as the risk of recurrence is not negligible.
Final diagnosis
Pulmonary hydatid disease.
Discussion
Echinococcus is caused by the larval stage of the cestode, Echinococcus, belonging to the family of Taeniidae.(1) These tapeworms are small and range in size from 2 to 12 mm in length. Humans are accidental intermediate hosts and acquire echinococcus through the faeco-oral route.(2) There are four main species known to cause disease in humans. Echinococcus granulosis causes cystic echinococcus in humans. Echinococcus multilocularis causes alveolar echinococcus, Echinococcus oligarthrus causes unicystic echinococcus and Echinococcus vogeli causes polycystic echinococcus. (1) E. granulosis has several genotypes and each genotype has distinct intermediate host preferences, has specific geographical distributions and not all cause disease in humans.(3)
Although 162 cases have been reported in Southern Africa, these were in the form of case reports of atypical presentations of cystic echinococcus such as in the heart and spine. As a result, these do not represent the true epidemiology of cystic echinococcus in South Africa. No epidemiological studies have been done in Southern Africa thus far.(4) A retrospective data analysis of the National Health Laboratory services showed an overall positivity rate of 17% from submitted samples testing for hydatid disease in the form of serology, microscopy and histopathology. The Eastern Cape had a rate of 30.4% followed by the North West at 19% and Northern Cape at 18%. Mpumalanga had a rate of 8.5%, followed by Gauteng at 10.7% and Limpopo at 13.9.(5) A review by Kayser reported 20 cases of hydatid disease in one Eastern Cape hospital, however the prevalence of hydatid disease of the lung in South Africa is unknown.(6)
Risk factors include poor water hygiene, slaughtering livestock close to humans and dogs, uncontrolled dog populations in close contact to sheep-raising communities as well as veterinarians and farmers. These risk factors are important to know for effective prevention and control of human echinococcus.(7)
Most patients with pulmonary hydatid disease have no symptoms as the cysts are slow growing. Pulmonary lesions are usually detected incidentally when performing chest imaging for another reason. Symptomatology depends on whether the cyst is intact or not, the location and size of the cyst.
Intact cysts are initially asymptomatic but enlarge at a rate of 1-50mm/year, thereby potentially causing compression of nearby structures and producing symptoms when large enough. Ruptured cysts present acutely with fever, pleuritic chest pain, and productive cough due to the ionic content of the cyst fluid, with grapelike membranes expectorated if rupture occurs into the bronchus. If the cyst ruptures into the pleural space it will result in a hydropneumothorax.(8, 9)
Pulmonary hydatid disease is diagnosed by a combination of suggestive lung imaging findings on chest radiograph, CT scan or MRI, and serology. This includes well circumscribed, homogenous radio-opacity on chest radiograph, which may take a strange shape due to pressure of the surrounding broncho-vascular structures. Crescent, cumbo and water lily signs due to varying amounts of air entering between the pericyst and endocyst layers are appreciated on CT scan. Serology in the form of either ELISA or indirect haemagglutination tests may be used.(10, 11)
Treatment of pulmonary hydatid disease is less well established than liver hydatid disease. Both pharmacological and surgical intervention can be attempted, depending on cysts size and location.
Medical treatment is preferred for small cysts (<5cm), multiple cysts in multiple lobes of the lung and if patients are poor surgical candidates. Medical treatment includes albendazole, praziquantel, or combination treatment of albendazole and praziquantel. Current recommendations from the Infectious Diseases Society of America, suggest use of albendazole therapy, however evidence for length of therapy is minimal.(12) Evidence for combination therapy with praziquantel is scarce and further evaluation is needed before recommendations are changed.(13, 14).
Bigger cysts (>5cm, especially >10 cm called giant cysts), cysts close to vital structures and infected cysts warrant surgical therapy. Pregnant patients in their first trimester and patients prone to bone marrow suppression may also be considered.(1) There are various surgical techniques used, however PAIR (Puncture, aspiration, instillation and re-aspiration) is not routinely done due to the risk of complications in the thoracic cavity.(1, 14, 15) The other surgical techniques include enucleation, cystotomy with capitonnage, segmental resection and lobectomy to mention a few. (16)
The monitoring of patients following surgery and on medical treatment is based on extrapolation from monitoring of patients with liver hydatid disease. This is in the form of imaging every 6 to 12 months for at least 5 years as the risk of recurrence can be 4.6-22%.(17) Serology is not used for monitoring as antibody titres may remain positive for years following successful treatment.(18)
Recommended reading
1.Brunetti E, Kern P, Vuitton DA. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta tropica. 2010;114(1):1-16.
2.Morar R, Feldman C. Pulmonary echinococcosis. European Respiratory Journal. 2003;21(6):1069-77.
3.Velasco-Tirado V, Alonso-Sardón M, Lopez-Bernus A, Romero-Alegría Á, Burguillo FJ, Muro A, et al. Medical treatment of cystic echinococcosis: systematic review and meta-analysis. BMC infectious diseases. 2018;18(1):306.
4.Garg MK, Sharma M, Gulati A, Gorsi U, Aggarwal AN, Agarwal R, et al. Imaging in pulmonary hydatid cysts. World journal of radiology. 2016;8(6):581-7.
References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®