
Tom Boyles, Marc Mendelson - Department of Infectious Diseases and HIV Medicine, Division of Medicine, UCT.
Case presentation
27 year old man from the Philippines presented to a peripheral hospital in Cape Town with a 1 week history of fever, headache, chills and euritic chest pain. He also had a cough productive of blood stained sputum. Six weeks earlier he had left his job as a rice farmer in Northern Philippines and flown to Montevideo where he immediately boarded a cargo ship bound for Cape Town. He remained fit and well for the first 5 weeks of the journey while working on the ship and only became sick 1 week prior to arrival. He had no other previous travel history and no previous illnesses of note. Initial CXR (figure 1) showed some ill-defined opacification of the lung fields bilaterally with a pleural effusion and he was treated with ceftriaxone and clarithromycin for community acquired pneumonia. Four sets of blood cultures taken after initiation of antibiotics were subsequently negative.
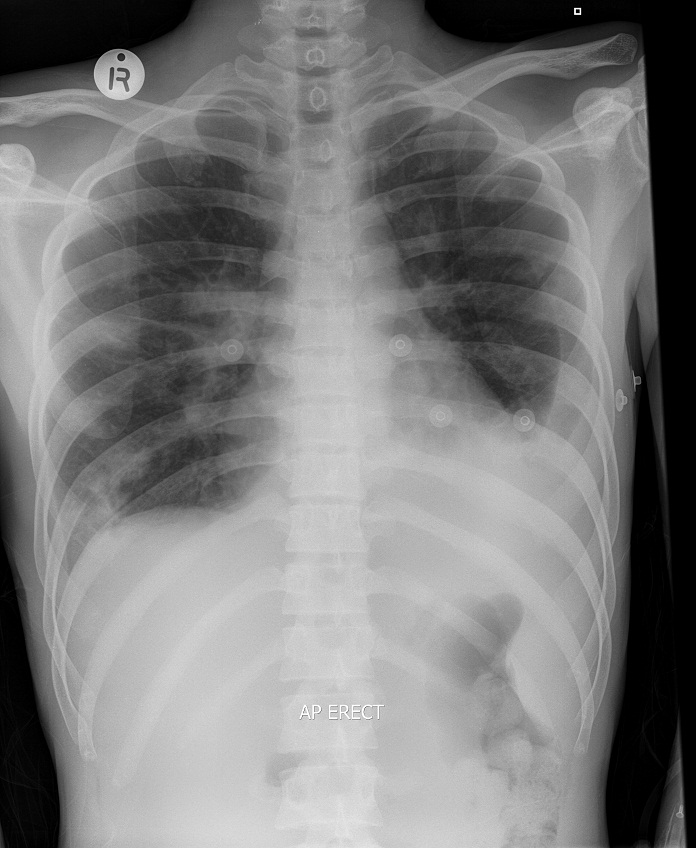
Figure 1
Symptoms did not improve and he was transferred to our institution after 4 days. At this time he was unwell with temperature 38.5 C, bibasal crepitations, a left pleural rub and a 5cm hepatomegaly. Investigations showed total WCC 11, Hb 11, plt 39, bil 312, ALT 226, ALP 116. HIV serology was negative, sputum smear microscopy with ZN stain was negative on 2 occasions. The pleural aspirate was neutrophil predominant (60%) with a total protein of 44, LDH 1057, ADA 16,6 and both bacterial and mycobacterial cultures were negative.
At this point a clinical diagnosis of melioidosis was made and imipenem 500mg 6hrly was initiated. After 4 days the fever had settled and the patient was feeling better and his blood parameters began to normalise. He continued to improve and after 14 days of imipenem he was discharged with a 3 month course of co-trimoxazole.
Question 1: Which organism causes melioidosis, what is its geographical distribution and route of transmission?
Answer to Q1
Melioidosis is caused by the aerobic, gram-negative motile bacillus Burkholderia pseudomallei. It is found in water and moist soil in South East Asia and Northern Australia where disease is endemic. Transmission is by inhalation, inoculation through broken skin or ingestion of the organism. Incidence rates are reported to be 16.5/100 000/yr in Northern Australia and 1.7/100 000/yr in Singapore although the greatest burden of disease is likely to be in Thailand, Malaysia, the Philippines and Indonesia. There have been reports of sporadic infection from other tropical areas including Northeastern Brazil, and East Africa.
Question 2: What are the risk factors for melioidosis?
Answer to Q2
Environmental risk factors are exposure to the organism particularly when working with water and soil in an endemic area eg rice farming. Individual risk factors include diabetes mellitus which is coincident in 50% of infections, renal disease, thalassaemia, alcoholism, immunosupressive drugs, chronic lung disease and consumption of kava which is a crushed vegetable root eaten uncooked. HIV is not a risk factor for melioidosis.
Question 3: What is the typical clinical presentation?
Answer to Q3
The median incubation period is thought to be around 9 days but can be much longer. Latent infection with reactivation also occurs and this has been described up to 62 years after initial exposure. The majority of infections are probably subclinical with the most common clinical presentation being either localised skin infection with or without abscesses or pneumonia. Around 50% of patients with pneumonia will become bacteraemic. More severe disease results from bacteraemic spread which can be to almost any site and when this occurs abscess formation is common. Typical sites of dissemination are the genitourinary system, bone, joints and the eye. Abscesses also from within organs such as the liver and spleen. A common presentation in children is suppurative parotitis.
Question 4: How is the diagnosis made and what is the recommended treatment?
Answer to Q4
efinitive diagnosis is based on positive culture for B. pseudomallei, although its distinctive “safety pin” appearance can also be seen on Gram stain. The sensitivity of culture is unknown and a clinical diagnosis may be made in a patient with the appropriate exposure history and compatible clinical syndrome. Appropriate specimens for culture are blood, sputum, urine, swab of an ulcer or skin lesion, abscess fluid, throat swab or rectal swab. Ashdown’s liquid transport broth should be used for transport if available although consultation with the local microbiology laboratory is advised if melioidosis is considered. B. pseudomallei is a biohazard level 3 pathogen.
Treatment is 2 weeks of -
Ceftazidime 2g ivi 6 hourly
Or
Imipenem 500mg ivi 6 hourly
Or
Meropenem 1g ivi 8 hourly
Followed by
Cotrimoxazole 960mg 12 hourly for 3 months
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
P.O. Box 16011,
Atlasville,
1465
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®