
Juanita Lishman, Lisa Frigati, Helena Rabie. Division of Pediatric Infectious Diseases, Department of Pediatrics and Child Health Stellenbosch University and Tygerberg Hospital
Juanita Lishman, Lisa Frigati, Helena Rabie. Division
of Pediatric Infectious Diseases, Department of Pediatrics and Child Health
Stellenbosch University and Tygerberg Hospital
A 2 year 10-month-old girl presents with a five-day history of a fever and a runny nose, cough with post-tussive vomiting, and conjunctivitis.
She was previously well with no prior admissions. She was born at term; her immunizations were up to date and she was HIV unexposed. There were no contacts at home with tuberculosis or COVID-19 and no household smokers. There was also no history of atopy.
On initial examination she was tachycardic and tachypnoeic with oxygen saturation of 91% in room air. She had signs of respiratory distress including alar flare, intercostal and subcostal recession. On auscultation of her lungs she had bilateral inspiratory crepitations and a soft expiratory wheeze. The rest of the assessment was normal.
Low flow oxygen was initiated and the saturation improved. Further management included oral antibiotic and inhaled B2agonist – to which she was responsive.
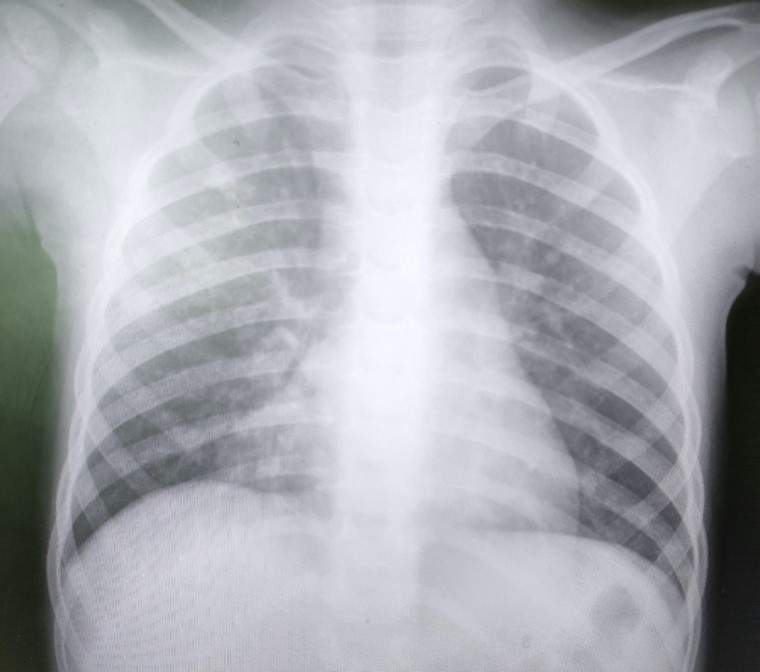
Chest X-ray (Fig 1) showed bilateral infiltrates with air bronchograms, most prominent in the right upper and middle lobe. C-reactive protein that was slightly elevated at 26mg/L with a normal white Cell Count of 9.21 x 109/L. Her HIV test was negative.
Fig 1: Chest radiograph of 2 year 10-month-old girl with severe lower respiratory tract infection.
Question 1: Which pathogens would you consider as part of the differential diagnosis in this infant?
The clinical features suggest a viral lower respiratory tract infection, the season and circulating pathogens should be considered to establish the most likely cause, but includes:
Other pathogens to consider include Streptococcus pneumoniae, Hemophilus influenza pertussis and mycoplasma. Pertussis like coughing, as was noted in this child, is not unique to Bortetella pertussis and Bortetella parapertussis, but has also been associated with viral infection including adenovirus, as well as bacterial infections including Streptococcus pneumoniae.
Nasopharyngeal aspirate was sent for viral PCR panel was positive for adenovirus
Adenoviruses are nonenveloped double- stranded DNA viruses that were first isolated in 1953 as part of a project searching for the virus causing the common cold. There are currently over 60 recognized serotypes of human adenovirus, which can be divided into the subgroups (or species) A to G. There are increasing reports of virus persistence particularly in the tonsils and intestinal lymphoid tissue and this may play a role in disease in immune suppressed patients and presents a diagnostic conundrum if patients test repeatedly postive. Prolonged shedding in the respiratory and gastrointestinal tract in immune competent children are also well described.
Adenovirus is spread by droplet infection, direct contact with infected secretions, and via the faecal-oral route. It can remain viable for prolonged periods on environmental surfaces and is not susceptible to some commonly used disinfectants. Handwashing is usually recommended for this reason but hand rubs based with high ethanol concentration or isopropyl alcohol do have viricidal activity against adenovirus. Infection prevention and control is crucial and numerous healthcare associated outbreaks have been reported.
Question 2: Describe the adenoviral syndromes and their associated serotypes
Adenovirus subgroups A and F typically cause infection of the gastrointestinal tract, and subgroups B, C and E shows tropism for the respiratory tract. Epidemic kerato- conjunctivitis is predominantly caused by serotypes of subgroup D.
Typical clinical presentations of adenovirus include pharyngoconjunctival fever. This syndrome typically affects children more than adults and presents with acute onset high fever, pharyngitis and conjunctivitis that initially affects one eye and then 3-4 days later the other eye becomes involved. Outbreaks can occur in childcare facilities and swimming areas. Epidemic keratoconjunctivitis is more common in adults and has a slower onset with simultaneous bilateral eye involvement. Adenovirus, types 40 and 41 have been associated with gastroenteritis as well as intussusception.
Pneumonia, as in this case, is often more severe in children and can lead to a need for respiratory support and even death in previously healthy children. The white cell count and CRP in children with adenovirus can be raised and this therefore may be confused with a bacterial infection. Adenovirus is by far the most common cause of post-infectious bronchiolitis obliterans in children. In these children mechanical ventilation is an independent risk factor to develop post-infectious bronchiolitis obliterans. In addition, adenovirus is commonly found in the lower airways of children with protracted bacterial bronchitis and bronchiectasis suggesting a role in the development of chronic lung disease in children without cystic fibrosis as well as a role in symptom exacerbation in children with established bronchiectasis.Adenovirus is common cause of viral myocarditis, in some reports up to 60% of cases are attributed to adenovirus.
Question 3: Does Adenovirus cause hepatitis?
Adenovirus hepatitis has been described in paediatric liver transplant recipients and other immunocompromised children, the cause is usually species C serotype 5. Adenovirus 41 has also been detected in some cases of acute hepatitis in immunocompetent children. Slight elevations in ALT are reported in young children with adenovirus, enterovirus and RSV associated lower respiratory tract infections.
Currently there is a concern of an increase in severe unexplained hepatitis in children in Europe and North America. Many of these children progressed to liver transplant or death. In 70% of these children adenovirus (in particular 41) was found, but is not clear what role, if any adenovirus plays, currently theories include:
The WHO case definition is the following:
The majority of children are < 5 years of age without known co-morbidities. In a case series of 9 children from Alabama, USA all 9 children had adenovirus on PCR in the blood, but 7 patients also had evidence of other viral infections, and liver biopsy in 6 children did not illustrate inclusion bodies.
A quick refence and notification guide for the South African context can be found at:
https://www.nicd.ac.za/wp-content/uploads/2022/05/Acute-Hepatitis-Quick-Reference-Final-30-05-2022.p... . The local case definition is slightly different excluding Hepatitis D and E. In children that meet the case definition the NICD will test specimens for adenovirusQuestion 4: How Can adenovirus be diagnosed?
Diagnosis is mostly made using a PCR assay on a nasopharyngeal aspirate or swab, throat swab, sputum sample, or bronchoalveolar lavage fluid. PCR can also be performed on urine, stool, CSF as well as histological specimens. This allows for rapid diagnosis of adenovirus.
In tissues, characteristic intranuclear inclusions can be noted and the virus identified on electron microscopy or through immunohistochemistry.
Other strategies include viral antigen assays these are test of choice for serotype 40 and 41 and culture, the latter is no longer routine.
Question 5: What is the treatment of adenovirus?
Treatment is usually supportive but cidofovir has been shown to have some effect against adenovirus. Intravenous immune globulin can be considered in immune compromised children with conflicting data on its utility in immune competent children with severe pneumonia.
Question 6: How can the spread of Adenovirus be prevented?
A live oral vaccine against serotypes 4 and 7 was used by the US military
In other settings the main stay of prevention remains good prevention and cleaning practice.
The Committee on Infectious Diseases of the American Academy of Pediatrics recommends the following:
References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
P.O. Box 16011,
Atlasville,
1465
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®