
Elmi Barnard¹, Jan Loot Pretorius¹, Kessendri Reddy²
¹ Worcester Hospital, Internal Medicine
² Division of Medical Microbiology, Stellenbosch University and Tygerberg Hospital
Case presentation
A 28-year-old male patient presented in August 2020 with a two-month history of left tempo-parietal headache, change in sleeping pattern, social withdrawal and gait instability. He had no known comorbidities and recently tested HIV negative. He was referred to Worcester Hospital in September 2020 for a CT Brain.
Examination of the patient revealed multiple soft-tissue masses on the scalp and abdominal wall. He had a slight hemiparesis on the right. Chest examination revealed a prominent left parasternal heave with no other signs of pulmonary hypertension or right ventricular failure.
Fourth generation HIV ELISA was negative.
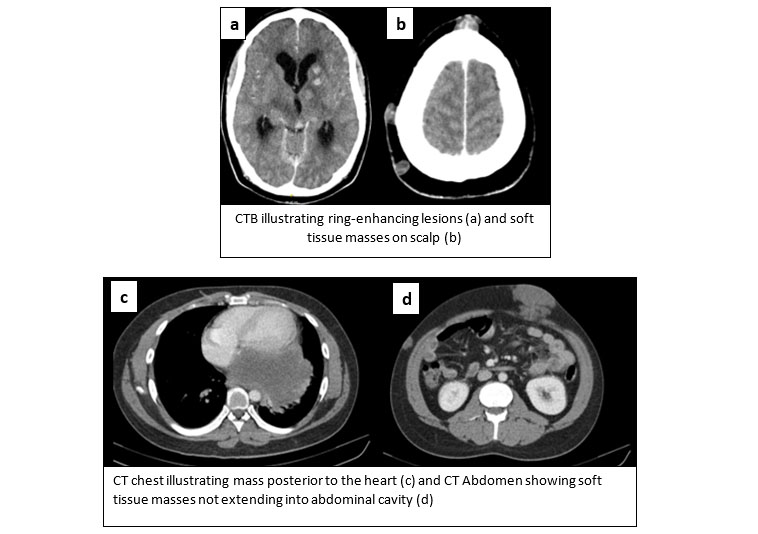
Contrasted CTB showed left basal ganglia ring enhancing lesions and an ill circumscribed right cerebellar mass resulting in non-communicating hydrocephalus (Image a). CT chest revealed a 12cm left lower lobe solitary mass abutting the heart posteriorly, which could explain the prominent parasternal heave resulting from anterior displacement of the heart and increased contact area of the right ventricle with the sternum (Image c). Multiple subcutaneous collections were also evident (Images b and d).
Assessment at this point was that of an ostensibly immunocompetent male presenting with ring-enhancing lesions in the brain and cutaneous as well as thoracic masses. Differential diagnosis included:
Malignancy:
1. Bronchus carcinoma with metastasis
2. Lymphoma
Infection:
1. Tuberculosis
2. Nocardia
3. Disseminated fungal infection:
1. Histoplasmosis
2. Blastomycosis
3. Cryptococcosis
Aspiration of the cutaneous masses revealed a gel-like fluid (image e) that showed moderated yeast cells on microscopy. Culture identified Cryptococcus gattii species.
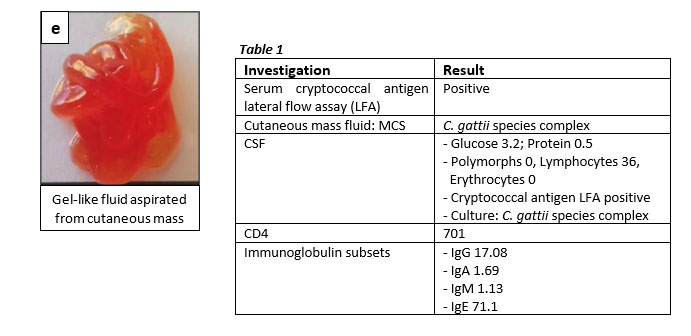
A lumbar puncture was performed with an opening pressure of > 50cmH2O. CSF showed a lymphocyte predominant pleocytosis, cryptococcal antigen LFA positive and culture confirmed C. gattii.
CD4 count was within normal limits that excluded idiopathic CD4 lymphopaenia. Immunoglobulin subsets were also normal.
A diagnosis of disseminated C. gattii complicated by meningoencephalitis with central nervous system, cutaneous and pulmonary cryptococcomas was made.
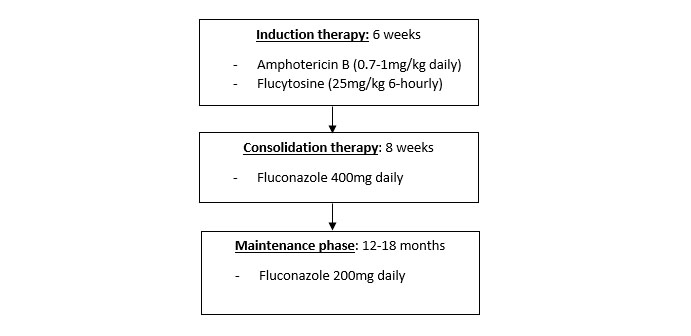
The patient was initiated on Amphotericin B (75mg daily intravenous), Flucytosine (1.75g 6hourly per os) and short course steroid therapy (prednisone 60mg daily per os). He was transferred to Tygerberg Hospital Neurosurgery where a ventriculoperitoneal shunt was inserted to address the hydrocephalus. He completed 6 weeks of Flucytosine and Amphotericin B and was then initiated on Fluconazole maintenance therapy (400mg daily per os).
Discussion:
C. gattii is a basidiomycetous fungus found in the environment. In the current HIV-pandemic, C. neoformans has been regarded as the more prevalent fungal infection causing cryptococcosis. This case gives us the opportunity to gain knowledge regarding the difference in presentation and management of the less common C. gattii, an important emerging fungal pathogen that also affects immunocompetent individuals. There are limited data available regarding the incidence of C. gattii in South Africa as well as the incidence in the HIV infected compared to the HIV uninfected population. One South African study in Gauteng that looked at cryptococcal infection during the 2002-2004 period, reported that only 2.4% of cases of cryptococcal meningoencephalitis could be ascribed to C. gattii. Of these patients, the majority (61%) was found to be HIV infected, 37% had unknown HIV status compared to 2.2% that was confirmed HIV negative (Morgan et al). Another South African study that observed cryptococcal infections in the paediatric population found that children were significantly more likely than adults to be infected with C. gattii, 9 vs. 3% (Meiring et al). Important to note however, is the prevalence of C. gattii might be higher than currently estimated since the laboratory diagnosis of C. gattii can be challenging (See laboratory aspects of Cryptococcus identification, below).
What is the natural reservoir of C. gattii?
C. gattii is a fungal pathogen that is endemic in the tropics, subtropics and temperate climatic regions, such as Australia, South America, South East Asia and Sub Saharan Africa. Environmental reservoirs of C. gattii are plant and wood debris. The infection has been associated with exposure to certain trees, in particular, eucalyptus trees.
There is a lack of data on the environmental distribution of C. gattii in South Africa.
Is cryptococcal disease only for the immunodeficient?
Compared to the more common C. neoformans, which typically cause disease in immunocompromised hosts, a significant proportion of cases of C. gattii infection are detected in immunocompetent hosts. However,conditions that impair immunity such as HIV, malignancy, organ transplantation, glucocorticoid therapy, idiopathic CD4 lymphopenia, sarcoidosis and chronic lung disease seem to be linked to a higher incidence of C. gattii infection.
How does the clinical presentation between C. gattii and C. neoformans differ?
C. gattii infection most commonly involves the central nervous system and the lungs. Other systems that could be affected include the skin, eyes, soft tissues, bones, joints, bone marrow, larynx and lymph nodes. The involvement of multiple systems could be independent of the host’s immune status.
C. gattii is similar to C. neoformans as neurologic infections manifest most often as potentially fatal meningoencephalitis. Patients may present with headache, neck-stiffness and other neurological deficits (including focal neurological fallout, delirium and seizures).
Pulmonary involvement can present with cough, dyspnoea and chest pain and manifests either as a pneumonia or with pulmonary nodules/cryptococcomas.
Cutaneous cryptococcosis can occur as part of disseminated C. gattii disease or as primary skin disease due to inoculation. Areas typically affected by skin lesions include the face and neck and morphology of disease range from papules, pustules, ulcers, subcutaneous masses or cellulitis.
C. gattii infection is much more likely to cause a disproportional number of large mass lesions (cryptococcomas) in the central nervous system and/or the lungs compared to C. neoformans, as was the case in our patient.
Severe neurological sequelae such as seizures, focal neurology and ocular complications including papilledema, visual field defects, extra-and intraocular muscle paresis, uveitis, optic atrophy and blindness have been reported more frequently in C. gattii infections.
Similar to C. neoformans, raised intracranial pressure (CSF > 20cm H2O) is a common complication of C. gattii, presenting with symptoms such as headache, papilledema and neurological deficits such as abducens nerve palsy. Raised intracranial pressure can either be due to meningitis or due to cryptococcomas causing mass effect and obstructive hydrocephalus, as was the case in our patient.
Current evidence regarding the mortality and long-term neurological sequelae in C. gattii and C. neoformans infected patients are also very limited, but the long-term impact on morbidity and mortality seems to be high. Data ranges from 13 to 33% mortality in a non-HIV infected C. gattii-infected cohort to 78% in an HIV-infected cryptococcal meningitis cohort (Chen et al & Pasquier et al). A South-African study found that C. gattii was associated with a high mortality (35.6%), but it was not significantly different from the mortality of non-gattii infections (Morgan et al) whereas an Australian study identified significantly higher gattii-related mortality in immunocompromised patients (29%) than in healthy hosts (0.04%) (Chen et al). C. gattii-related cryptococcomas hold more long-term neurological sequelae compared to C. neoformans meningoencephalitis. Factors influencing mortality include the immune status of the patient, organ systems involved and the timing and type of treatment regimen given.
Making the diagnosis of C. gattii infection:
Investigations necessary to diagnose C. gattii infections are very similar to investigations for C. neoformans infections. There are, however, a few specific differences:
Laboratory aspects of Cryptococcus identification:
Distinguishing between the closely-related C. neoformans and C. gattii can be challenging at a routine diagnostic laboratory level. The CrAg lateral flow assay (IMMY, Oklahoma, USA) is an important tool in the national reflex cryptococcal antigen screening programme and is widely used in South Africa, but cannot differentiate between these two species. Automated identification systems commonly used in diagnostic laboratories in the public sector may accurately identify C. neoformans, but occasionally cannot discriminate between different Cryptococcus species, necessitating the use of supplementary identification methods.
Further identification tests to discriminate between C. neoformans and C. gattii include serotyping, use of the chromogenic CGB (L-canavanine, glycine, bromothymol blue) agar and molecular methods. These methods have various advantages and disadvantages, but are not generally part of the routine diagnostic workflow in the public sector in South Africa where the overwhelming majority of isolates belong to the C. neoformans group.
Antifungal susceptibility testing is not standardized and is not routinely available.
Because of these limitations in the general laboratory testing approach, it is crucial that clinicians and laboratory personnel are vigilant to the possibility of C. gattii infection in the appropriate clinical setting, and that the specimen/isolate is flagged for additional testing. The Centre for Healthcare-Associated Infections, Antimicrobial Resistance and Mycoses at the National Institute of Communicable Disease is the reference laboratory in our setting and provides assistance with laboratory aspects of identification and susceptibility testing, as well as clinical advice where needed.
How does the treatment between C. gattii and C. neoformans differ?
There are no randomized trial data with regard to treatment of C. gattii infection and current recommendations for the management are based on expert opinion.
Where the treatment regimen for C. neoformans is dependent on the immune status of the host, the decision regarding the regimen and duration of therapy in C. gattii depends on the sites involved and the presence or absence of cryptococcomas.
Generally, management will include:
1) Antifungal treatment:
- An induction course of Amphotericin B and flucytosine followed by consolidation and then maintenance therapy with fluconazole
- Induction course in C. gattii infection is longer in duration compared to induction course in C. neoformans infection, and ranges from 2 weeks for isolated pulmonary disease to 6 weeks for CNS involvement. Induction phase is generally prolonged with CNS involvement and in the presence of cryptococcomas.
- According to the 2010 Clinical Practice Guideline for the Management of Cryptococcal Disease by the Infectious Disease Society of America, a 4-week induction course can be given for a person with meningoencephalitis, given that there is no neurological complications and that a repeat LP after 2 weeks of treatment, shows a negative yeast culture result.
- Duration of maintenance phase is also prolonged in C. gattii and can range from 12-18 months in CNS disease. The total duration depends on clinical response to treatment.
- A repeat CT is recommended to monitor response to treatment or if the patient has worsening CNS symptoms.
- It is important to improve immunity to prevent relapse: initiate antiretroviral treatment in the HIV-infected individual or address other reversible causes of immunosuppression.
2) Control of intracranial pressure:
Treatment directed at lowering intracranial pressure and thus preventing secondary brain damage is critical in improving clinical outcomes in C. gattii CNS infection. Daily lumbar puncture is recommended until pressure is below 250 mmH2O and symptoms are stabilised for two consecutive days. Surgical intervention to relieve pressure, by means of lumbar percutaneous drains or ventriculoperitoneal shunts, are recommended if the pressure remains high with daily lumbar punctures or if the patient has obstructive hydrocephalus.
3) Role of glucocorticoids:
Case studies have shown limited success
with adjunctive glucocorticoids when CNS cryptococcomas are associated with
significant oedema and accompanying neurological deficit and should be
considered if both are present. Prednisone 0,5 to 1mg/kg/d initially with a
taper over 2 to 6 weeks.
4) When to consider surgical resection of cryptococcomas?
Few studies exist that address indications for surgical intervention and there are no clinical trials on which to base the timing of resection during antifungal treatment. Surgical resection of cryptococcomas could be considered in the following instances:
1) Therapeutic indications:
a. Single large lesion, especially when accessible and complicated by mass effect of surrounding vital structures and perilesional oedema.
b. To improve the response to antifungal therapy. Cryptococcomas can respond slowly to antifungal treatment largely due the large fungal burden as well as the tendency of C. gattii to infect immunocompetent hosts with resultant immune reconstitution inflammatory syndrome.
c. Surgical excision should also be considered for enlarging symptomatic lesions in spite of adequate antifungal therapy.
2) Diagnostic indications:
a. When there is doubt about whether a mass lesion represents an infectious disease or malignancy.
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
P.O. Box 16011,
Atlasville,
1465
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®